Download
1 / 30
380 likes | 1.09k Vues
ABYLCAP CARBON DIOXIDE REMOVAL ECCO 2 R. TREATMENTS FOR CO 2 REMOVAL. WHY ?. Low tidal volume High tidal volume. During the use of mechanical ventilation with low tidal volume, the exceeding CO 2 arising from this “protective” technique is to be removed to avoid Acidosis.

E N D
Low tidal volume High tidal volume During the use of mechanical ventilation with low tidal volume, the exceeding CO2 arising from this “protective” technique is to be removed to avoid Acidosis .
ARF (Acute Respiratory Failure) It’s an alteration in alveolar ventilation and / or a difficulty in pulmonary gas exchange, which can be determined by insufficient transport of oxygen to the tissues or by insufficient utilization of oxygen by peripheral tissues ARDS (Acute Respiratory Distress Syndrome) ARDS is a severe acute respiratory failure resulting from pulmonary edema caused by increased permeability of the alveolar capillary barrier. ARDS is a specific lung disease, it is rather a severe pulmonary dysfunction due to underlying lung disease (sepsis, trauma, pneumonia).
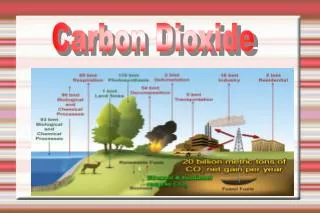
Brain How is CO2 distributed? Heart • CO2 spreads from tissues and is moved to the alveolar capillaries in 3 different ways: • from about 3 to 5% in a physically diluted form (solubility 0,00069 mL/mL/mmHg) • from about 7 to 10% bound to the Hb through a carbaminic bind (carbo-hemoglobin) • More than 80% “interacts” in the red blood cell to turn into HCO3- in the plasmatic water Kidney
7-10% 3-5% CO2 CO2 CO2 CO2 85-90% Caboemoglobina CO2 + H2O ca H2CO3 } HCO3- HCO3- H+ HHb Cl- Cl- } Hb K+ Na+ HbO2 O2 O2 O2 O2 H2O H2O Tissues Plasma Red blood cell Capillary wall Cl-
How does CO2 move “through” the red blood cells? Spreading from the tissues into the red blood cells, the CO2 catalyzes the hydration reaction through carbonic anhydrase: CO2 + H20 -> H2CO3 • Then it dissociates: H2CO3 -> H+ + HCO3- • The hydrogen ion (H+) is buffered by the Hb, the bicarbonate ion (HCO3- ) moves from the red blood cell into plasma through a carrier protein of the erythrocyte membrane, simultaneously an exchange takes place with a chloride ion (Cl-)
CO2 CO2 CO2 CO2 Caboemoglobina } HCO3- HCO3- H+ HHb Cl- Cl- } Hb K+ Na+ HbO2 O2 O2 O2 O2 H2O H2O Lung Plasma Red Blood Cell Capillary wall CO2 + H2O ca H2CO3
How is CO2 expelled ? The adverse reaction arises when the blood oxygenation causes an increase in the acidity of Hb and it involves the following: • A decrease in the buffer capacity with a release of ionsH+ • Hence: H+ + HCO3- -> H2CO3 -> H20 + CO2. • And the CO2 in excess is released
How is CO2 expelled ? A decrease in the strength of the carbaminic binds between Hb and CO2 allows the release of CO2 by 7-10% transferred in the form of carbo-hemoglobin • Inside capillaries the effect leads to a higher intake of CO2 in blood because O2 is released from Hb • Inside pulmonary alveoli the effect leads to a higher output of CO2 from blood due to the fact that the Hb binds with O2
The inclination of the solubility curve between 40 and 45 mmHg is 0,0045 (mL/mL)/mmHg Less than half of CO2 released in lungs is due to the 5 mmHg excursion down the venous dissociation curve. The release of the remaining CO2 occurs due to the downwards shift of the dissociation curve, meaning the Haldane effect occurring when the pO2 changes from 40 mmHg (75% of O2 saturation) to 100 mmHg (100% O2 saturation)
The total quantity of CO2 in blood is proportional to its partial pressure
The factors that shift the dissociation curve of Hb With the same value of pO2 we have greater or lesser percentage of saturation of Hb
The factors that shift the dissociation curve of Hb With the same value of pO2 we have greater or lesser percentage of saturation of Hb
Ossigenator O2 CO2
Characteristics The kit is made up of: • 2 couples of Lines for extracorporeal circulation • 2 heating Lines • 1 Lilliput ECMO 2 Oxygenator • Connectors
Main characteristics • Lilliput ECMO2 Oxygenator • Polymethylpentene membrane • Membrane surface 0,67 m2 • Heater surface 0,02 m2 • Filling volume 90 ml • Connections 1/4”- 5/16” • Maximum flow 2300 ml/min • 5 days duration • ETO Sterilization
ECMO Vs CPB ECMO CPB Duration Characteristics of materials More than 21 days Maximum 3,5 h
Plasma-tight membrane: POLYMETHYLPENTENE Fibres in Polypropylene: gas comes into contact with blood through microporous fibres. The gas transfer is obtained through direct contact. Polypropylene “standard“ membrane Fibres in Polymethylpentene: the hollow fibres are protected by an external thin membrane. Gas transfer is obtained by diffusion. Polymethylpentene “plasma-tight“ membrane
Polypropylene “standard“ fibre Polymethylpentene “plasma-tight“ fibre Plasma-tight membrane: POLYMETHYLPENTENE OUTER SURFACE Main technical characteristics: • Gas transferred by diffusion (no direct contact blood gas) • No plasma-breakthrough (>120h, according to Dideco test procedures) • Gas exchange capacity compared to other hollow fibers that work in direct contact(for the protection of the external surface 1 mm) • Suitable for long-lasting use
1) resorption of HCO3- 2) regeneration of HCO3-.
APPLICATION IN INTENSIVE CARE Lynda is the first example of multidisciplinary approach CPFA Treatment for patients with severe sepsis, septic shock or MOF Intermittent Treatments for Renal Failure Continuous Treatments for Renal Failure Therapeutic Plasma Exchange Treatments Treatments for CO2 Removal
CONCLUSIONS Thanks to Lynda, Bellco can propose to the I.C. Units a “multi-organ support therapy”by integrating in one single device a support for: ECCO2R Ventilation, TPE Plasma exchange, CVVH, CVVHD, CVVHDF Acute Renal Failureand CPFA Sepsis.