Download
1 / 36
360 likes | 383 Vues
This study explores the impact of congenital hypogonadism on sexuality and quality of life in women with Turner's Syndrome and other forms of hypogonadism. The study examines the etiology, comorbidities, and management of these conditions, as well as their effects on psychological and neural profiles.

E N D
Sexuality and Quality ofLife in CongenitalHypogonadisms Camil Castelo-Branco Hospital Clínic. University of Barcelona
Turner’sSd. MultidisciplinaryTeam • Department of Endocrinology • Irene Halperin • Dept. Psychiatry • Esther Gómez • Teresa Godás • Department of Cardiology • Paula Dantas • Steroidslab • GregoriCasals
Populations who may experience female sexual dysfunction (FSD): • Abused • Perimenopausal • Pregnancy • Multiple sclerosis • Childhood sex abuse • Chemotherapy • Genital mutation • Post menopausal • Lack of sensitivity • Gynecological cancer • Radiation • Battered • Neurogenic disease • Sexual trauma • Spinal cord injury • Vascular disease • Post-hysterectomy • Post-partum (Brassil et. al, 2002)
Statistics Different epidemiologic studies on FSD suggested that up to 49% of women experienced sexual dysfunction. Blümel JE, Castelo-Branco C et al. Menopause. 2004;11(1):78-81. Castelo-Branco C, Blumel JE, et al.J Obstet Gynaecol. 2003 Jul;23(4):426-30. TS represent < 0.03% General population Castelo-Branco C. Maturitas. 2014 Dec;79(4):471-5. Ros C & Castelo-Branco C. Gynecol Endocrinol. 2012 Sep;28(9):726-32. US population data revealed that 9.7 million women (50-74 y) self-report complaints of diminished vaginal lubrication, pain and discomfort with intercourse, decreased arousal, and difficulty achieving orgasm. Berman J et al. Urology. 1999;54(3):385-91
Etiology “The etiologies of female sexual dysfunction affect a variety of populations and may be caused by psychological, emotional, or physiological reasons. Often, the etiology is multifactorial & interrelated.” Castelo-Branco C et al. Expert Opin Ther Patents. 2007;17(6):639-647
Etiology: Psychological Causes As with most disorders, female sexual dysfunction can be caused and aggravated by psychological causes. • (Sexual or) Emotional Abuse • Depression • Relationship Issues • Stress • Self Esteem
Turner’sSyndrome (TS) TS is the most common chromosomal abnormality in females, and affects one in 2500 live female births. This condition is more common in utero, affecting 1–2% of all conspectuses. TS is the result of the absence or the abnormality of the second sexual chromosome, in at least one cellular line.
Turner’s Syndrome (TS) Ros C & Castelo-Branco C. Gynecol Endocrinol. 2012 Sep;28(9):726-32
TS: Cardinal features • Gonadal dysgenesis (ovarian failure) • Short stature • Dysmorphology
Women with TS have a highrisk of developinghealthproblemsfromchildhoodtoadulthood. GYNECOLOGIST: HORMONE THERAPY REPRODUCTIVE COUNSEIL COMORBIDITIES MANAGEMENT REFER TO OTHER SPECIALISTS Multidisciplinary management: ENT, Rheumatologist, Genetist, Cardiologist, Neurologist, Nephrologist,… • Congenital malformations • Early comorbidities • hGH & HT Comorbiditiesthat debut orimpair in adultages Pediatricages
TS: Comorbidity • Osteoporosis • Cardiovascular diseases • Metabolic abnormalities • Immunological disorders • Sensorineural disorders • Kidney malformations • Psychosocial development
Other Congenital Hipogonadisms Ross JL, Stefanatos GA, Kushner H, Zinn A, Bondy C, Roeltgen D. Persistent cognitive deficits in adult women with Turner syndrome. Neurology. 2002;58:218-25. Schmidt PJ, Cardoso GMP, Ross JL, Haq N, Rubinow DR, Bondy CA. Shyness, social anxiety, and impaired self-esteem in Turner syndrome and premature ovarian failure. JAMA 2006;295:1374-6.
TS: Psychoneural profile Naess EE et al (2010). Health status in women with Turner syndrome: a questionnairestudy on healthstatus, education, workparticipation and aspects of sexual functioning. Clin Endocrinol
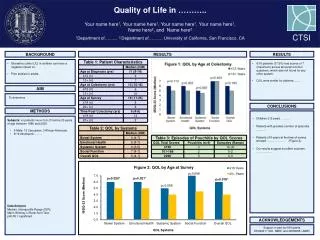
TS: Impairment of QoL and sexual function Ros C, Alobid I, Balasch J, Mullol J, Castelo-Branco C (2013). Turner's syndrome and other forms of congenital hypogonadism impair quality of life and sexual function Am J Obstet Gynecol. 2013 Jun;208(6):484.e1-6
TS: Impairment of QoL and sexual function Ros C, Alobid I, Balasch J, Mullol J, Castelo-Branco C (2013). Turner's syndrome and other forms of congenital hypogonadism impair quality of life and sexual function Am J Obstet Gynecol. 2013 Jun;208(6):484.e1-6
TS: Impairment of QoL and sexual function Castelo-Branco C (2016). Quality of life and sexual function in Turner's syndrome and other forms of congenital hypogonadism Unpublished data
TS: Quality of Life (SF-36) Bannink EM, Raat H, Mulder PG de Muinck Keizer-Schrama SM. Quality of life after growth hormone therapy and inducedpuberty in women with Turner syndrome. J Pediatr 2006;148:95–101
PF RP BP GH VT SF RE MH TS: Quality of Life (SF-36) p=0,026 * p=0,032 * p=0,025 † p=0,05 † p=0,027 †
TS: Quality of Life (SF-36) Naess EE, Bahr D, Gravholt CH. ClinEndocrinol 2010;72:678–84.
TS: Quality of Life (SF-36) AGE Naess EE, Bahr D, Gravholt CH. Clin Endocrinol 2010;72:678–84.
TS: Quality of Life (SF-36) ENT Carel JC, ET Al. J ClinEndocrinolMetab 2006; 91:2972-9
TS: Quality of Life (SF-36) TS vs OCH 100/103 100/128 35 Schmidt PJ, et Al. JAMA 2006;295:1374-6.
TS: Sexual function (FSFI) 98 TS karyotype 37 years (18-59 y) Derogatis Interview for Sexual Functioning 30% sexual active Percentile 10th Sheaffer A, Lange E, Bondy C. J Womens Health 2008;17:27-33
TS: Sexual function (FSFI) Sheaffer A, Lange E, Bondy C. J Womens Health 2008;17:27-33
TS: Sexual function (FSFI) 168/80/51 Naess EE, Bahr D, Gravholt CH. ClinEndocrinol 2010;72:678–84.
TS: Sexual function (FSFI) Castelo-Branco C (2016). Quality of life and sexual function in Turner's syndrome and other forms of congenital hypogonadism. Unpublished data
TS: Sexual function 566 Carel JC, ET Al. J ClinEndocrinolMetab 2006; 91:2972-9
TS: Sexual function Carel JC, ET Al. J ClinEndocrinolMetab 2006; 91:2972-9
TS: Sexual function (FSFI) †p=0.001 †p=0.013 †p=0.007 • *p=0.009 †p=0.02