Download
1 / 56
560 likes | 638 Vues
Learn about pulse oximetry screening for newborns, its benefits, and potential obstacles. Understand the importance of early detection of critical congenital heart disease through non-invasive and low-cost screening methods.

E N D
Pulse Oximetry Screening An Introduction to Advocacy Issues
Agenda • The Nuts and Bolts of Screening, Dr. Paul Matherne • Overview of Benefits and Potential Obstacles, Dr. John Hokansen • Update a Federal Landscape, Annamarie Saarinen • Grassroots Advocacy, Saiza Elayda • Questions
Pulse Oximetry Screening The Nuts and Bolts of Screening G. Paul Matherne MD, MBA Professor of Pediatrics Division Head Pediatric Cardiology University of Virginia Health System
U United States 4,000,000 Births Per Year 40,000 Births All Congenital Heart Disease 10,000 Births Severe Congenital Heart Disease
The Nightmare • Some children with critical congenital heart disease will have no symptoms and have an entirely normal physical examination at the time they are sent home from the hospital after birth. • These children may become critically ill or die in the next few days if their congenital heart disease is not recognized. • It has been estimated, conservatively, that 100-200 babies each year may die from unrecognized critical congenital heart disease in the United States.
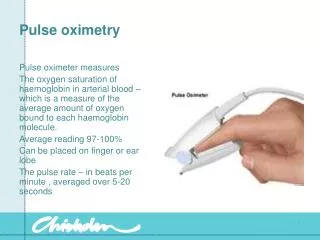
Pulse Oximetry Screening Is: • An assessment of oxygen level to check for cyanosis in newborns before they leave the hospital. • Low blood oxygen levels may indicate the presence of congenital heart defects or other serious health conditions.
Pulse Oximetry Screening Is: • Painless. It requires the application of a probe to the hand and foot. The probe does not puncture the skin. • Quick. A measurement can be read in 30 to 60 seconds. • Simple. It is easy for all healthcare personnel to perform. • Low Cost Supplies. Disposable or reusable probes are inexpensive.
Pulse Oximetry Screening Is: • Life-saving. Early detection can save lives. • Disability-reducing. Early intervention can prevent or reduce disability. • The right thing to do.
Pulse Oximetry Screening Overview of Benefits and Potential Obstacles John S. Hokanson, MD Pediatric Cardiologist, Faculty University of Wisconsin School of Medicine and Public Health
What will screening involve? • Minimal inconvenience for most patients • Moderate inconvenience for occasional patients • Significant inconvenience for a few patients • Life saving for a handful of babies
What happens if a baby fails the screening process? • The next logical step is to perform an echocardiogram before sending the baby home. • When same-day neonatal echocardiography is not available, a decision to extend the hospitalization or to transfer the baby to a center where an echocardiogram can be performed must be made. • The availability of neonatal echocardiography is critical to the planning for any large scale pulse oximetry screening project.
Other Issues • The best data comes from European studies, but there aren’t any large US studies. • A large US study is unlikely in the foreseeable future. • No studies have been done in very small nurseries, much less in home delivery or birthing center settings. • Any screening program has costs and risks. • Unfortunately, we don’t know as much about how screening would work as we would like.
Pulse Oximetry • Strengths • Adds one last safety net for a couple hundred babies a year in the US. • Oximetry devices are cheap, non-invasive and ubiquitous in hospitals. • Even the two-site protocols are fairly straight forward. • Weaknesses • Will not detect all forms of congenital heart disease. • False positives and negatives will occur. • The main costs are incurred by the follow-up testing to the oximetry screening.
Strengths of Pulse Oximetry • The costs of the oximeter and the nursing time required are low. • The screening is non-invasive (harmless). • Pulse oximetry screening can detect babies with critical congenital heart disease that will otherwise be missed AND who will suffer harm due to the missed diagnosis. • The defects detected by oximetry are those most likely to lead to death and disability if unrecognized.
Weakness of Pulse Oximetry • Any screening costs money. • Pulse oximetry will not detect many serious, although not immediately life threatening heart defects. • A great deal of cost and anxiety are incurred every time a child fails the screening. All will be forgiven if the a catastrophe is prevented, but there may be backlash if the baby is normal after all. • This screening is difficult to complete in settings where echocardiography is not immediately available.
Mandated Screening • May increase rate of screening and the uniformity of screening • May meet resistance from hospital groups • May be difficult for Midwives or others doing home deliveries • May allow for tracking and quality assurance in a way that is probably not possible for screening which is recommended but not required
Follow the Money • Pulse Oximeter <$1,000 per device $ • Nursing Time to perform screening $ • Echocardiography >$1,000 per study $$$
Follow the Money • Pulse Oximeter <$1,000 per device $ • Nursing Time to perform screening $ • Echocardiography >$1,000 per study $$$ • Transport • 50 miles by ambulance >$5,000 $$$$ • 50 miles by helicopter >$10,000 $$$$$ • Cardiology clinic visit >$250 $$ • Evaluation in ER >$500 $$$ • One night in hospital >$1,500 $$$ • Telephone call to pediatric cardiology Free
Preliminary Data from a Survey of Neonatal Care in Wisconsin Dan Beissel MD John S. Hokanson MD University of Wisconsin
Pediatric Cardiology Practices
Wisconsin as an example of how pulse oximetry screening might work in the real world • Wisconsin is a rural state with many small nurseries. • Some of these nurseries are more than 100 miles from the nearest level II NICU. • Some of these nurseries are 200 miles from the nearest pediatric cardiac surgery center.
Wisconsin 2002-2006 • Babies discharged as normal newborns who were hospitalized or died due to unrecognized critical congenital heart disease in the first two weeks after birth • Death or Hospitalization • 1 in 24,684 births 3 per year in WI • Death • 1 in 38,397 births 2 per year in WI
2009 Wisconsin Birth Statistics • 60,421 Hospital Births in survey hospitals • 99 Hospitals did deliveries, 88 responded • 25 Hospitals had 250 to 500 deliveries • 35 Hospitals had less than 250 deliveries • Typically there are 1,000 birthing center and home births per year in Wisconsin.
2011 February-March Survey • At present 1/3 of the babies born in Wisconsin undergo pulse oximetry screening for congenital heart disease. • At present 2/3 of the babies born in Wisconsin are born in a setting where same-day neonatal echocardiography is available. • The average distance required to transport a baby to a facility with echocardiography was just over 50 miles when same day echocardiography was not available.
A year in America’s Dairyland when all babies are screen with oximetry • 65,000+ babies pass the screening with minimal inconvenience • 10-100 babies fail the screening test? • 5 or so have unrecognized severe CHD • All the rest turn out to be normal, but 1/3 of these will have to leave the place where they were born to get an echocardiogram.
Going Forward • Pulse oximetry does provide a valuable last safety net for a small group of babies. • An effective strategy will be one which can practically be performed in all settings in which babies are born. • Screening is currently underway as a huge uncontrolled experiment and tracking of the results is a vital piece of the equation.
Update on Federal Landscape Newborn Screening for Critical Congenial Heart Defects Using Pulse Oximetry Annamarie Saarinen
Federal Landscape • Unprecedented support • Public Health Need • Patient Access to Specialty Care
Federal Recommendation Hurdles: Public Health As a point of care evaluation – this screening is only the second of its kind, and the first to detect a birth defect. Hurdles to state by state adoption include: Infrastructure needs Uniform screening technologies and protocols Diagnostic follow up Health information exchange Reporting and surveillance Standards and education
Federal Recommendation Hurdles: Access Newborns and infants represent the largest patient transfer population in health care. Less than 3% of the nation’s hospitals have onsite pediatric specialty services.Babies are born at community hospitals representing the remaining 97%.Only 150 facilities can address cardiac conditions in infants.Transport and referral guidelines are essential: majority of US hospitals do not have on-site pediatric echo capability, would need to transfer.
More about the SACHDNC:http://www.hrsa.gov/heritabledisorderscommittee/More about the SACHDNC: Workgroup on Screening for Critical Congenital Cyanotic Heart Diseasehttp://altarum.cvent.com/events/ccchd-meeting/custom-22-f8929dc795694e7aa6c588c263e31554.aspx SACHDNC letter to Secretary Sebelius Recommending Newborn Screening for CCHD http://www.hrsa.gov/heritabledisorderscommittee/correspondence/October15th2010letter.htm Statement from AAP New Jersey on Pulse Oximetry screening: http://pulseoxadvocacy.com/wp-content/uploads/2011/07/Bill-A3744-1.pdf
Grassroots Advocacy Saiza Elayda American College of Cardiology seylada@acc.org
Grassroots Advocacy – What is it? • To effect change • Citizen-driven movement • Bottom-up approach
Grassroots Advocacy – Why is it important? • No participation = no right to blame • Necessary for change to occur • Responsibility to participate
State vs. Federal Grassroots • Different session lengths • Different timeline for bill introduction • More accessible • Focused more on local issues
Define your objective • New local initiative? • Introduce legislation? • Initiate regional program?
Know the Opposition • Identify opponents and their motivation • Be prepared to respond • Is there common ground?
Build Grassroots Support • Recruitment forums • Explain the issue and position • Articulate why the issue is important to you and to them • Get commitments for support • Discuss strategy and resources • Mobilize at critical moments • Provide support and appreciation
Research • Determine your audience • Understand where your audience stands • Prior actions • Know the issues and facts • Understand possible impacts • Look at results from other communities
Messaging • Develop and deliver a central message • Make the issue personal
Message Mode • How will the message be sent? • Email? • Letter? • Phone call? • Personal visit?
Scheduling a Meeting • Call the appropriate office in advance • Realize that the average meeting will last between 5 to 15 minutes
Leave Behind • Prepare materials to leave behind • Sharp, punchy bullets • Include contact information
Close the Deal • At the end of your meeting, be direct. Can we count on you for your support?
Follow-Up • Send a “Thank You” note • Offer additional information/resources • Maintain communication • Keep your legislator apprised of events that your organization is having in his/her district. • Attend town halls and other local events • Make yourself known
Resources • 1in100.org • pulseoxadvocacy.org • advocacy@mendedlittlehearts.org