Monitoring Pulse Oximetry
Monitoring Pulse Oximetry. By the EMT-Basic. Objectives. Understand the Indiana Regulations relative to monitoring pulse oximetry by the EMT-B/A Review the signs and symptoms of respiratory compromise Understand the importance of adequate tissue perfusion

Monitoring Pulse Oximetry
E N D
Presentation Transcript
Monitoring Pulse Oximetry By the EMT-Basic
Objectives • Understand the Indiana Regulations relative to monitoring pulse oximetry by the EMT-B/A • Review the signs and symptoms of respiratory compromise • Understand the importance of adequate tissue perfusion • Define hypoxia and describe the clinical signs and symptoms
continued • Describe the technology of the pulse oximeter • Define normal parameters of oxygen saturation • Describe the relationship between oxygen saturation and partial pressure oxygen • Describe the significance of the information provided by pulse oximetry • Describe monitoring pulse oximetry during patient assessment
continued • Describe the use of pulse oximetry with pediatrics • Describe patient conditions that may affect pulse oximetry accuracy • Describe patient environments that may affect pulse oximetry accuracy • Describe the evaluation and documentation of pulse oximetry monitoring
Kansas Regulations • Indiana EMS Regs: • Adopts “EMT-Basic Advanced Initiatives” • Allows EMTs to monitor saturation of arterial oxygen levels of blood by way of pulse oximetry • Appropriate physician oversight • On line medical control or written protocols • Complete a course of instruction
Respiratory Compromise • Signs and Symptoms • Dyspnea • Accessory muscle use • Inability to speak in full sentences • Adventitious breath sounds • Increased or decreased breathing rates • Shallow breathing • Flared nostrils or pursed lips
continued • Retractions • Upright or tripod position • Unusual anatomy changes
Hypoxemia • Decreased oxygen in arterial blood • Results in decreased cellular oxygenation • Anaerobic metabolism • Loss of cellular energy production
Hypoxemia Etiology • Inadequate External Respiration • Decreased on-loading of oxygen at pulmonary capillaries • Inadequate Oxygen Transport • Decreased oxygen carrying capacity • Inadequate Internal Respiration • Decreased off-loading of oxygen at cellular capillaries
External Respiration • Exchange of gases between the alveoli and pulmonary capillaries • Oxygen diffuses from an area of higher concentration to an area of lower oxygen concentration • Oxygen must be available and must be able to diffuse across alveolar and capillary membranes • Oxygen must be able to saturate the hemoglobin
Inadequate External Respiration • Decreased oxygen available in the environment • Smoke inhalation • Toxic gas inhalation • High altitudes • Enclosures without outside ventilation • Inadequate mechanical ventilation • Pain • Rib fractures • Pleurisy
continued • Traumatic injuries • Open pneumothorax • Loss of ability to change intrathoracic pressures • Crushing injuries of the neck and chest • Traumatic asphyxia • Crushing neck injuries • Tension pneumothorax • Increased intrathoracic pressures reducing ventilation • Hemothorax • Blood in thoracic cavity reducing lung expansion • Flail Chest • Loss of ability to change intrathoracic pressures
continued • Other conditions • Upper Airway Obstruction • Epiglottitis • Croup • Airway Edema-anaphylaxis • Lower Airway Obstructions • Asthma • Airway Edema from inhalation of toxic substances
continued • Hypoventilation • Muscle Paralysis • Spinal injuries • Paralytic drug for intubation • Drug Overdose • Respiratory depressants • Brain Stem Injuries • Damage to the respiratory center
continued • Inadequate oxygen diffusion • Pulmonary edema • Fluid between alveoli and capillaries inhibit diffusion • Pneumonia • Consolidation reduces surface area of respiratory membranes • Reduces the ventilation-perfusion ratio • COPD • Air trapping in alveoli • Loss of surface area of respiratory membranes
continued • Pulmonary emboli • Area of the lung is ventilated but hypoperfused • Loss of functional respiration membranes
Oxygen Transport • Most of the oxygen in arterial blood is saturated on hemoglobin • Red blood cells must be adequate in number and have adequate hemoglobin • Sufficient circulation is necessary to transport oxygen to the cellular level
Inadequate Oxygen Transport • Anemia • Reduces red blood cells reduce oxygen carrying capacity • Inadequate hemoglobin results in the loss of oxygen saturation • Poisoning • Carbon monoxide on-loads on the hemoglobin more readily preventing oxygen saturation and oxygen carrying capacity • Shock • Low blood pressures result in inadequate oxygen carrying capacity
Internal Respiration • Exchange of gases from the systemic capillaries to the tissue cells • Oxygen must be able to off-load the hemoglobin • Oxygen moves from a area of higher concentration to an area of lower concentration of oxygen
Inadequate Internal Respiration • Shock • Oxygen is not available due to massive peripheral vasoconstriction or micro-emboli • Cellular environment is not conducive to off-loading oxygen • Acid Base Imbalance • Lower than normal temperature • Poisoning • CO will reduce the oxygen available at the cellular level
Signs and Symptoms of Hypoxemia • Restlessness • Altered or deteriorating mental status • Increased or decreased pulse rates • Increased or decrease respiratory rates • Decreased oxygen oximetry readings • Cyanosis (late sign)
Pathophysiology • Oxygen is exchanged by diffusion from higher concentrations to lower concentrations • Most of the oxygen in the arterial blood is carried bound to hemoglobin • 97% of total oxygen is normally bound to hemoglobin • 3% of total oxygen is dissolved in the plasma
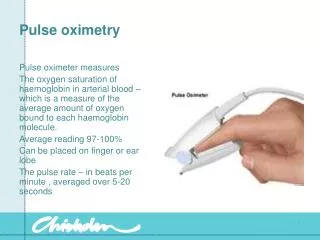
Oxygen Saturation • Percentage of hemoglobin saturated with oxygen • Normal SpO2 is 95-98% • Suspect cellular perfusion compromise if less than 95% SpO2 • Insure adequate airway • Provide supplemental oxygen • Monitor carefully for further changes and intervene appropriately
continued • Suspect severe cellular perfusion compromise when SpO2 is less than 90% • Insure airway and provide positive ventilations if necessary • Administer high flow oxygen • Head injured patients should never drop below 90% SpO2
SpO2 and PaO2 • SpO2 indicates the oxygen bound to hemoglobin • Closely corresponds to SaO2 measured in laboratory tests • SpO2 indicates the saturation was obtained with non-invasive oximetry • PaO2 indicates the oxygen dissolved in the plasma • Measured in ABGs
continued • Normal PaO2 is 80-100 mmHg • Normally • 80-100 mm Hg corresponds to 95-100% SpO2 • 60 mm Hg corresponds to 90% SpO2 • 40 mm Hg corresponds to 75% SpO2
Technology • The pulse oximeter has Light-emitting diodes (LEDs) that produce red and infrared light • LEDs and the detector are on opposite sides of the sensor • Sensor must be place so light passes through a capillary bed • Requires physiological pulsatile waves to measure saturation • Requires a pulse or a pulse wave (Adequate CPR)
continued • Oxygenated blood and deoxygenated blood absorb different light sources • Oxyhemoglobin absorbs more infrared light • Reduced hemoglobin absorbs more red light • Pulse oximetry reveals arterial saturation my measuring the difference.
Patient Assessment • Patient assessment should include all components • Scene Size-up • Initial Assessment • Rapid Trauma Assessment or Focused Physical Exam • Focused History • Vital Signs • Detailed Assessment • Ongoing Assessment
Pulse Oximetry Monitoring • Pulse oximetry monitoring is NOT intended to replace any part of the patient assessment • Pulse oximetry is a useful adjunct in assessing the patient’s oxygenation and monitoring treatment interventions • Initiate pulse oximetry immediately prior to or concurrently with oxygen administration
Continuous Monitoring • Monitor current oxygenation status and response to oxygen therapy • Monitor response to nebulized treatments • Monitor patient following intubation • Monitor patient following positioning patients for stabilization and transport • Decreased circulating oxygen in the blood may occur rapidly without immediate clinical signs and symptoms
Pediatrics • Use appropriate sized sensors • Adult sensors may be used on arms or feet • Active movement may cause erroneous readings • Pulse rate on the oximeter must coincide with palpated pulse • Poor perfusion will cause erroneous readings • Treat patient according to clinical status when in doubt • Pulse oximetry is useless in pediatric cardiac arrest
Conditions Affecting Accuracy • Patient conditions • Carboxyhemoglobin • Anemia • Hypovolemia/Hypotension • Hypothermia
Carboxyhemoglobin • Carbon monoxide has 200-250 greater affinity for the hemoglobin molecule than oxygen • Binds at the oxygen binding site • Prevents on-loading of oxygen • Fails of readily off-load at the tissue cells • Carboxyhemoglobin can not be distinguished from oxyhemoglobin by pulse oximetry • Erroneously high reading may present
continued • Suspect the presence of carboxyhemoglobin in patient with: • Smoke inhalation • Intentional and accidental CO poisoning • Heavy cigarette smoking Treat carboxyhemoglobin with high flow oxygen irregardless of the pulse oximetry reading!
Anemia • Low quantities of erythrocytes or hemoglobin • Normal value of hemoglobin is 11-18 g/dl • Values as low as 5 g/dl may result in 100% SpO2 Anemic patients require high levels of oxygen to compensate for low oxygen carrying capacities!
Hypovolemia/Hypotension • Adequate oxygen saturation but reduced oxygen carrying capacity • Vasoconstriction or reduction in cardiac output may result in loss of detectable pulsatile waveform at sensor site • Patients in shock or receiving vasoconstrictors may not have adequate perfusion to be detected by oximetry Always administer oxygen to patients with poor perfusion!
Hypothermia • Severe peripheral vasoconstriction may prevent oximetry detection • Shivering may result in erroneous oximetry motion • Pulse rate on oximeter must coincide with palpable pulse rate to be considered accurate Treat the patient according to hypothermic guidelines and administer oxygen accordingly!
Patient Environments • Ambient Light • Excessive Motion
Ambient Lighting • Any external light exposure to capillary bed where sampling is occurring may result in an erroneous reading • Most sensors are designed to prevent light from passing through the shell • Shielding the sensor by covering the extremity is acceptable
Excessive Motion • New technology filters out most motion artifact • Always compare the palpable pulse rate with the pulse rate indicated on the pulse oximetry • If they do not coincide, reading must be considered inaccurate
Other Concerns • Fingernail polish and pressed on nails • Most commonly use nails and fingernail polish will not affect pulse oximetry accuracy • Some shades of blue, black and green may affect accuracy (remove with acetone pad) • Metallic flaked polish should be removed with acetone pad • The sensor may be placed on the ear if reading is affected
continued • Skin pigmentation • Apply sensor to the fingertips of darkly pigmented patients.
Interpreting Pulse Oximetry • Assess and treat the PATIENT not the oximeter! • Use oximetry as an adjunct to patient assessment and treatment evaluation NEVER withhold oxygen if the patient ahs signs or symptoms of hypoxia or hypoxemia irregardless of oximetry readings!
continued • Pulse oximetry measures oxygenation not ventilation • Pulse oximetry does NOT indicate the removal of carbon dioxide from the blood!
Documentation • Pulse oximetry is usually documented as SpO2 • Distinguishes non-invasive pulse oximetry from SaO2 determined by laboratory testing • Document oximetry readings as frequently as other vital signs • When oximetry reading is obtained before oxygen administration, designate the reading as “room air”
continued • When oxygen administration is changed, document the evaluation of pulse oximetry • When treatments provided could potentially affect respiration or ventilation, document pulse oximetry • Spinal immobilization • Shock position • Fluid administration
Summary As with all monitoring devices, the interpretation of information and response to that interpretation is the responsibility of a properly trained technician!
References Bledsoe, B. et al. (2003). Essentials of paramedic care. Upper Saddle River, New Jersey: Prentice Hall. Halstead, D., Progress in pulse oximetry—a powerful tool for EMS providers. JEMS, 2001: 55-66. Henry, M., Stapleton, E. (1997). EMT prehospital care (2nd ed.). Philadelphia: W.B. Saunders. Limmer, D., et al. (2001) Emergency Care (9th ed.). Upper Saddle River, New Jersey: Prentice Hall. Porter, R., et al: The fifth vital sign. Emergency, 1991 22(3): 127-130. Sanders, M., (2001). Paramedic textbook (rev. 2nd ed.). St. Louis: Mosby. Shade, B., et al. (2002). EMT intermediate textbook (2nd ed.). St. Louis: Mosby. Cason, D., Pons, P. (1997) Paramedic field care: a complaint approach. St. Louis: Mosby.