Cardio ESA Stem
Cardio ESA Stem. What factor influence exchange of substances between capillaries and surrounding tissue Area available for exchange – capillary density Diffusion barrier Concentration gradient How is equilibrium between plasma and interstitial fluid generated Starling forces

Cardio ESA Stem
E N D
Presentation Transcript
What factor influence exchange of substances between capillaries and surrounding tissue • Area available for exchange – capillary density • Diffusion barrier • Concentration gradient • How is equilibrium between plasma and interstitial fluid generated • Starling forces • Hydrostatic pressure • Colloid oncotic pressure
What are the 3 histological layers of large blood vessels • Tunica intima – endothelial cells • Tunica media – smooth muscle • Tunica adventitia – CT • 3 types of capillaries • Continuous • Fenestrated • discontinuous
Describe the conducting system of the heart • Sino-atrial node • Atrioventricular node • Bundle of His • Bundle branches • Purkinje fibres
What is the blood supply to the heart • Coronary arteries • Left coronary artery • Left anterior descending coronary artery • Left circumflex • Right coronary artery • Posterior descending • These are often referred to as end arteries, what are end arteries • Sole blood supply to an area
What is the function of the pericardium • Protection of the heart • What are the 3 layers of the pericardium • Fibrous • Parietal • visceral
What properties of cardiac muscle allow it to operate as a pump • Doesn’t tire • Acts as functional syncytium • Conduction allows co-ordinated pattern of contraction • Organised into figure of 8 bands
Regulation of heart valve opening in cardiac cycle • Onset systole – ventricles begin to contract • Rise in intraventricular pressure causes backflow of blood towards atria – closes AV valves • Ventricles contract isovolumetrically and pressure rises • When intraventricular pressure > arterial presuresemilunar valves open – ejection of blood • When intraventricular pressure < arterial presurebackflow of blood closes semilunar valves • When intraventricular pressure < atrial pressure AV valves open and ventricle fill • Cycle repeats
What is the mediastinum • Cavity between the pleural cavities • What are the divisions and contents of each • Superior • Great vessels and nerves to arms • Posterior • Posterior descending vessels • Oesophagus • Trachea • Azygous and hemiazgous • Vagus nerve • Thoracic duct • Lymph nodes • Middle • Heart and pericardium • Anterior • Thymus • Lymphatic vessels and nodes • Internal mammary artery
Types of flow • Laminar • Turbulent • Factors increasing turbulence • High velocity • Low viscosity • Large diameter vessel • What is the relationship of flow to diameter of a vessel • Flow α r4
What factors affect resistance of blood vessels • R = Pressure gradient/flow • What is the effect of combining resistances • In series • Increase (add) • Parallel • Decrease
what is total peripheral resistance • Resistance of all blood vessels in the body • What vessels contribute most to this • Arterioles • How do you calculate mean pressure • 2/3 diastolic + 1/3 systolic • Cardiac output x total peripheral resistance
Why is compliance of arteries important for blood pressure • Converts intermittent flow into pulsatile flow • What is autoregulation • Intrinsic tendency of an organ/tissue to adjust blood flow in accordance with it’s metabolic need • How is autoregulation achieved • Increased metabolism = increased production of vasodilator metabolites = vasodilation = increased flow • Increased flow = washes away metabolites = decreased • 3 examples of vasodilator metabolites • H, K, adenosine, CO2
Explain Starling’s law of the heart • Increased venous return = increased EDV = increased SV • Energy of contraction = function of length of muscle fibres • Increased stretch = increased force of contraction • What does this law allow • Matches output of heart to input
What is pre-load • Mechanical state of heart at end of diastole • The magnitude of vol/pressure stretching ventricle • What is after-load • Resistance L ventricle must pump against • TPR • What are the effects of increased TPR on the heart • Increased afterload • Decreased SV (harder to eject blood) • Increased EDV (unchanged preload) = increased stretch • increased contractility • SV recovers
What is the bainbridge reflex • Increased venous pressure/volume • Sensed by atrial sense receptors • Visceral afferents to medulla oblongata • Visceral efferents (ANS) to heart • Increased HR
Describe the ventricular action potential • Phase 0 – rapid depolarisation • Rapid influx of Na through voltage-gated Na channels • Phase 1 – Na refractory period • inactivation of Na channels • Phase 2 – plateau • Voltage gated L-type Ca channels open • Phase 3 – repolarisation • Voltage gated K channels – opened by depolarisation but delayed opening • Phase 4 – resting membrane potential
What is meant by refractory period • Period during which another AP cannot be initiated • Absolute – Na channel inactive – cannot be reopened • Relative – Na channels can only be opened by v. Strong AP
Describe the action potential of pacemaker cells • Never reach rest • Membrane potential drifts upwards (pacemaker potential) until reaches threshold • Depolarisation • Na influx via non-selective cation channels • Ca influx via T-type Ca channels (open transiently) • Repolarisation • K channels
Name the 5 special circulations and their key features • Pulmonary – low pressure supply driven • Coronary – flow almost exclusively diastole • Increased HR = decreased diastolic time therefore less time for more need • Skin – mostly influenced by thermoregulation • Brain – virtually constant – strong autoregulation • Muscle – β2 receptors cause vasodilation on increased sympathetic activity
What is the response of the cardiac system to ingestion of food • Increased blood flow to GIT • Decreases TPR = decreased afterload • decreased arterial pressure sensed by barorecptors • Visceral afferents to medulla oblongata • Increased sympathetic stimulation of the heart • Increased contractility and HR • increased CO = restore arterial pressure
What is the cardiovascular response to exercise • Onset of exercise preceded by increased HR • Influence of cerebral cortex via medulla • Blood flow redistributed to skeletal muscle at expense of GIT and kidney • Brain constant and skin increases • Increased CO = increased venous return = increased HR (cope with volume)
What is the cardiovascular response to posture change from lying down to standing • Gravity = increased pooling of blood in legs • Increased transmural pressure of superficial veins of legs • Transient decreased central venous pressure • Decrease in CO • Decrease arterial pressure • Sensed by baroreceptors (feedback to medulla) • Increase HR/Contractility/venomotor tone/TPR • Maintain perfusion of vital organs over expense of others • If insufficient = postural hypotension
Describe the cardiovascular response to haemorrhage • Immediate • Decreased arterial pressure • Baroreceptor reflex • Increase HR/contractility/venomotor tone (recruit venous reservoir) • Intermediate (autotransfusion) • Decreased BP • Decreased hydrostatic pressure (< colloid oncotic pressure) • Fluid moves from ECF to blood • Longterm • Restore ECF – ADH and RAAS • Restore haematocrit – increased erythropoietin • Restore plasma proteins - liver
Describe the cardiovascular response to longterm increase in blood volume • Increased venous pressure = increased EDV • Increased CO • Increased arterial pressure • Wash away vasodilator metabolites • Autoregulation = increased TPR • Further compounds increased BP
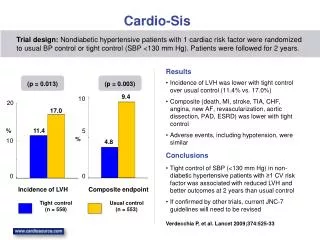
Why is it important to diagnose hypertension early • Short-term – effects are reversible • Long-term – remodelling of vessel walls leads to irreversible hypertension
What are the effects of sympathetic stimulus on the different components of the cardiovascular system • SA node – increase HR (rate of APs) • AV node – increased HR • increased automaticity and decreased delay in AP transmission to ventricles • Myocardium – increased contractility of ventricles and atria • Blood vessels – increased vasoconstriction • What receptors are activated • Β adrenergic
What are the effects of parasympathetic stimulus on the different components of the cardiovascular system • SA node – decrease HR (rate of APs) • Heart always under vagal tone (natural HR 100) • AV node – decreased HR • Decreased automaticity and increased delay in AP transmission to ventricles • Myocardium – decreased contractility of atria • No innervation to ventricles • Blood vessels – no innervation
On ECG, what do each of the letters stand for • P – atrial depolarisation • QRS – ventricle depolarisation • T – ventricle repolarisation • Why is there no atrial repolarisation • It’s masked by ventricle depolarisation
Which ECG lead normally records the largest R wave • Lead II • What does a shifting of the largest R wave to lead I indicate • Left ventricular hypertrophy • What does a shifting of the largest R wave to lead III indicate • right ventricular hypertrophy
How would the 3 types of heart block present on ECG • Right bundle block • M shaped R wave in V1, W shaped R wave in V6 • “marrow” • Left bundle block • W shaped R wave in V1, M shaped R wave in V6 • “william” • Complete heart block • No QRS complex
62yr old patient, Henry Walsh, attends GP clinic with a crushing central chest pain that gets worse with exercise and improves with rest. He has previously been diagnosed with hyperlipidaemia and is on statins. You suspect angina • What is the pathophysiology of angina • Insufficient blood flow to myocardium due to partial occlusion of coronary vessels • How could you confirm your diagnosis • Bloods – troponin (rule out MI) • Angiography (virtual or coronary) • Will you perform investigations in this case • No – typical Hx plus risk factors = treat as angina • Only investigate atypical cases
A year later Henry is rushed to A&E by ambulance with chest pain that is not remitting and is suspected to be having an MI • What investigations could (but probs won’t because patient would be dead) you do to confirm • Blood • Troponin • Creatininekinase • CRP • Lipid profile • ECG – looking for ST elevation, pathological Q waves • Inverted T-waves would appear after few days
19yr old Andrea Heskin is brought in with central chest pain • What is the differential diagnosis for chest pain • Cardiovascular • IHD, pericarditis, aortic dissection • Respiratory • Infection, PE, pneumothorax • GI • Reflux, oesophageal spasm • Musculoskeletal • Trauma, costochondritis
Andrea describes her pain as sharp and says it initially used to pass quickly but has become persistent. The pain is much worse when she takes a deep breath or is lying flat so she sits forward to relieve the pain. There’s nothing abnormal in her Hx except that she is just getting over a bout of gastroenteritis. • What is your suspected diagnosis • Acute pericarditis • What might you expect to hear on auscultation • Pericardial rub • What is the likely cause • Complication of her gastroenteritis
30yr old Charlie Marchal is rushed to A&E with a sudden onset “tearing” central chest pain radiating to his back and left shoulder that remains constant no matter what he does. He is sweating profusely and has fainted twice in the ambulance on the way to A&E and say he feels nauseous • What is your suspected diagnosis • Aortic dissection • How will you confirm your diagnosis • Transoesophageal echo (the only 1 you’d actually have time for) • CT/MRI • Angiography • How will you treat Charlie • Medical Emergency!!! - surgery
35yr old Debbie Lupton, attends clinic for a follow-up after finishing her recent course of chemotherapy. She tells you she’s been feeling very tired and weak and feeling short of breath, especially at night. On examination you find that she has raised JVP, peripheral oedema, crackles in her lungs and hepatomegaly • What do you suspect is her diagnosis • Congestive heart failure • What is the pathophysiology of congestive heart failure • Decreased ability of the left ventricle to pump • Decreased CO • Increased LV preload = increased pulmonary venous pressure (heart dilates) • Increased pressure in pulmonary capillaries • Imbalance of starling forces • Build up of fluid in lung interstitum = pulmonary oedema • (dyspnoea and crackles) • Increased pulmonary vascular resistance – increased afterload on RV • Backlog of blood in systemic veins • Increased JVP • Peripheral oedema • hepatomegaly
List the 6 types of shock • Hypovolaemic • Cardiogenic • Septic • Mechanical • Anaphylactic • Neurogenic • What is the basic treatment of all shock • 02 • IV fluids (replace volume) • Treat cause
What is the response of the cardiovascular system to hypovolaemic shock • Decreased circulating volume • Decreased venous return • Decreased SV and CO (starling’s law) • Decreased BP – sensed by baroreceptors • Increased sympathetic activity • Increased HR/Vasoconstriction/contractility • BP remains normal until bottoms out by the quantity of blood loss
What is the response of the cardiovascular system to cardiogenic shock • Damage to LV • Decreased contractility • Decreased CO • Increased EDV • Pulmonary congestion/oedema • RV failure
What is the response of the cardiovascular system to septic shock • Endotoxin release = inflam mediators • Vasodilation and IV coagulation = decreased volume • Leaky capillaries • Blood pools in peripheries • Decreased venous return • Decreased CO • Decreased BP
What is the response of the cardiovascular system to anaphylactic shock • inflam mediators • Vasodilation and IV coagulation = decreased volume • Leaky capillaries • Blood pools in peripheries • Decreased venous return • Decreased CO • Decreased BP
What are the 3 main types/causes of mechanical shock • PE • Tension pneumothorax • Cardiac tamponade
51yr old Julie Heskin presents to A&E with sudden onset shortness of breath and pleuritic chest pain. There’s nothing remarkable in her Hx except that she has recently returned from visiting her daughter in Australia. • what is your suspected diagnosis • Pulmonary Embolism • What investigations will confirm your diagnosis • Pulmonary angiogram • D-dimer assay • How will you treat • Anti-coagulants • Thrombolysis if severe
22yr old Claire Marchal presents with sudden onset and progressively worsening shortness of breath. Examination reveals poor chest expansion on 1 side and deviation of her trachea and absent breath sounds on the same side. • What is your suspected diagnosis • Tension pneumothorax • What is you immediate action • Decompression of thorax – chest tube
28yr old Alex Heskin presents with sharp stabbing chest pain, and shortness of breath and feeling light-headed following receiving a kick to the chest in a kickboxing match • What is your suspected diagnosis • Cardiac tamponade – pericardium filling with blood • How will you confirm • Echocardiogram • How will you treat • Sub-xiphoidpericardiocentesis