Download
1 / 53
540 likes | 671 Vues
Use of computed tomography in the initial evaluation of anterior abdominal stab wounds. The American journal of Surgery.2011 Desember. Ali Fallahzadeh. Shahid Sadoughi university of medical science 1391/4/22. Abstract. Background

E N D
Use of computed tomography in the initial evaluation of anterior abdominal stab wounds The American journal of Surgery.2011 Desember
Ali Fallahzadeh Shahid Sadoughi university of medical science 1391/4/22
Abstract Background • The purpose of this study was to assess the ability of computed tomography (CT) to facilitate initial management decisions in patients with anterior abdominal stab wounds.
Methods • A retrospective review was conducted of patients with anterior abdominal stab wounds who underwent CT over 4.5 years. Any abnormality suspicious for intra-abdominal injury was considered a positive finding on CT.
Results • Ninety-eight patients met the study's inclusion criteria. Positive findings on CT were noted in 30 patients (31%), leading to operative intervention in 67%. Injuries were confirmed in 95% of cases, but only 70% were therapeutic. Ten patients had nonoperative management despite positive findings on CT, including 5 patients with solid organ injuries. One patient underwent operative intervention for clinical deterioration, with negative findings. No computed tomographic evidence of injury was noted in the remaining 68 patients (69%), but 1 patient was noted to have a splenic injury while undergoing operative evaluation of the diaphragm. All remaining patients were treated nonoperatively with success.
Conclusions • In patients with anterior abdominal stab wounds, CT should be considered to facilitate initial management decisions, as it has the ability to delineate abnormalities suspicious for injury.
Keywords • Computed tomography; • Anterior abdominal; • Stab wounds; • Penetrating trauma
Background • In the past 3 decades, there has been an abundance of literature continuing to evolve Shaftan's1 original 1960s concept of “selective conservatism” in the evaluation of abdominal stab wounds. Progressive technologic advances have championed this concept by demonstrating the advantages of cross-sectional imaging using computed tomography (CT) in the initial evaluation of these patients. The bulk of such data, however, is based on patients with posterior and flank injuries, while only a handful of articles cite specifically the presence and outcomes of anterior abdominal stab wounds (AASWs).
Background • Although it is widely accepted that patients demonstrating signs of hemodynamic instability, peritonitis, or evisceration should undergo timely exploratory laparotomy, the proper conservative evaluation in hemodynamically stable patients with AASWs remains indefinable despite the multitude of proposed clinical pathways. [2], [3] and [4] The goal of the present study was to devise our own clinical assessment strategy focused on the accuracy of CT in facilitating early management decisions in patients with AASWs.
Methods • After receiving institutional review board approval, a retrospective analysis was performed of all patients with AASWs admitted over a 4.5-year period to an urban level I adult and pediatric trauma center. Inclusion criteria for the patients were based on any patient with an AASW who underwent an initial evaluation with CT. The anterior abdomen was defined as the area from the nipple line superiorly, the inguinal creases inferiorly, and the anterior-axillary lines laterally
Methods • Within the study group, the evaluated variables included patient demographics, the presence or absence of alcohol intoxication, the number and location of stab wounds, the mechanism of injury (self-inflicted vs not), associated injuries (clinical and radiographic), interpretation of CT findings, change in management on the basis of computed tomographic findings, institution of treatment, and outcomes.
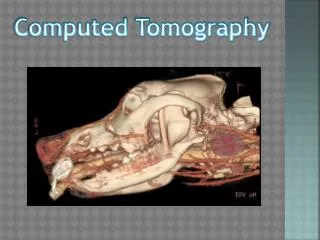
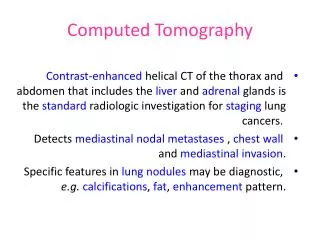
Methods • On the basis of attending physician preference, several patients underwent local wound exploration (LWE) as the initial evaluation. Positive findings on LWE were defined as the visualization of anterior fascial penetration. CT of the abdomen and pelvis was performed using a GE LightSpeed 16-slice system (GE Healthcare, Milwaukee, WI). Intravenous contrast (Isovue 360; Bracco Diagnostics, Princeton, NJ) was used in all cases, and the use of rectal and oral contrast (Omnipaque; GE Healthcare) was based on the attending surgeon's discretion
Methods • The images were acquired using a standard soft tissue algorithm with a slice thickness of 5 mm at 4-mm intervals. Coronal and sagittal reformats were made with 3-mm slices at 2-mm intervals. External markers were placed at the penetrating wound sites. Images were reviewed by a board-certified radiologist blinded to clinical symptoms or outcomes.
Methods • The results of CT were considered positive only if there were visible intra-abdominal findings suspicious of injury. The radiologist classified the abnormalities as solid organ injuries (SOIs), diaphragm irregularities, omental changes, or findings suspicious for hollow viscous injuries (HVIs), including pneumoperitoneum, free fluid without SOI, a track extending to the bowel wall, and/or mesenteric or bowel wall changes.
Methods • The depth of fascial penetration was interrogated and divided into 3 categories: superficial, intrafascial, or intraperitoneal. Superficial penetration included subcutaneous tissue depth, intrafascial penetration involved the abdominal musculature, and intraperitoneal extension was considered present if a visible tract was present extending into the peritoneum. Importantly, the presence of intraperitoneal extension of the stab wound without accompanying evidence of intra-abdominal injury was not classified as positive result on CT.
Methods • On the basis of the findings on CT, charts were reviewed to determine whether the patient would require operative intervention or clinical surveillance or could be discharge. Operative intervention was defined as therapeutic if there was a visceral injury that underwent surgical repair, as nontherapeutic if a visceral injury did not undergo surgical repair, and as negative if no injury was found. The isolated repair of a fascial defect did not constitute a therapeutic intervention in our study
Methods • Statistical analysis included determining the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of CT in diagnosing peritoneal violation (PV) and associated intra-abdominal injuries in the setting of AASWs.
Results • During the 4.5-year study period, 98 patients met the inclusion criteria. The patients were predominantly male (78%), with a mean age of 33 years (range, 11–68 years). Most patients sustained solitary stab wounds involving the upper quadrants. Almost 90% of the computed tomographic scans were performed after the administration of intravenous contrast material alone. There were no documented complications secondary to the use of CT.
Results • On assessment for intra-abdominal abnormalities, 30 patients (31%) had positive results on CT (Table 1). The likelihood of having positive findings on CT was not increased when multiple AASWs were present, if an AASW was not self-inflicted, or if rectal or oral contrast was administered for the study.
Results • On the basis of positive findings on CT, 20 patients were taken for operative intervention immediately (Fig. 1). In most cases, the decision to proceed to surgical intervention was based at least in part on concern for HVI (Table 2). In addition, operative intervention was more likely to be undertaken for SOIs when higher grades of injury were present (American Association for the Surgery of Trauma grade ≥ III) or if blush was seen on the initial CT.
Figure 1. Disposition of patients after abdominopelvic CT (apCT). IAI = intra-abdominal injury; OR = operating room.
Results • In 95% of cases, operative findings confirmed abnormalities seen on CT (Table 2), but therapeutic intervention was required in only 70% of cases (14 patients). Intraoperative findings confirmed preoperative suspicions in the 10 patients with HVIs, 5 patients with SOIs, and 2 patients with vascular injuries. Conversely, only 1 of 6 patients with diaphragm injuries noted on exploration had computed tomographic evidence of possible injury. Despite operative correlation of findings on CT, 5 patients underwent nontherapeutic intervention (Fig. 1).
Results • In this subgroup, surgical findings included a ruptured ovarian cyst, a pericolonic hematoma without an associated bowel injury, and cessation of bleeding from various sources. The single negative laparotomy occurred in a 68-year-old man with a self-inflicted stab wound to the right upper quadrant noted on CT to have a tiny amount of pneumoperitoneum and trace free fluid at the liver edge. Intraoperative findings were consistent with intra-abdominal penetration, but only a small hemoperitoneum was found, presumably from bleeding at the stab wound site.
Results • The remaining 10 patients had nonoperative management chosen, despite abnormalities noted on CT (Fig. 1). In 4 patients, findings on CT were not thought to be secondary to intra-abdominal injury: isolated minimal amounts of fluid (n = 3) and minute pneumoperitoneum beneath PV (n = 1). All were admitted for serial abdominal examination. Ultimately, 2 patients underwent negative laparotomy secondary to changes in examination. The remaining 6 patients had intra-abdominal findings consistent with traumatic injury after AASWs isolated to the right upper quadrant, but the decision was made to treat them nonoperatively.
Results • Hepatic injuries were diagnosed in 5 patients (grade II, n = 4; grade III, n = 1), and an additional patient had evidence of an omental hematoma. Within this group, no patient had evidence of hemodynamic compromise or required transfusion, and all were discharged without operative or radiographic intervention (Table 3).
Results • Sixty-eight patients had no evidence of intra-abdominal injury on CT (Fig. 1). Despite this, because of left upper quadrant locations of the AASWs, 10 patients underwent subsequent diagnostic laparoscopy to evaluate the diaphragm for possible injury. Although no diaphragmatic injuries were encountered, an actively bleeding grade I splenic laceration with minimal hemoperitoneum was revealed in 1 patient, which required intervention
Results • This patient was noted to be intoxicated on admission and had evidence of abdominal pain and tenderness isolated to the left upper quadrant. Additionally, 2 patients with isolated evidence of PV on CT were taken to the operating room on the basis of attending physician discretion, and each underwent negative laparotomy.
Results • Approximately 80% of the remaining patients with no evidence of abdominal injuries on CT required admission for reasons demonstrated in Table 4. Notably, the majority were found to need psychiatric evaluation secondary to the self-inflicted etiology of their wounds or because of additional injuries (pneumothorax or hemothorax [69%], cardiac injuries [13%]). No patient who was initially observed after negative findings on CT required delayed operative intervention. Importantly, of those without demonstrated reasons for admission, 71% (12 of 17) were discharged from the emergency department an average of 5 hours (range, 2–7.5 hours) after arrival.
Results • Data was available to correlate CT-assessed depth of abdominal wall penetration with LWE, evidence of SOI on CT, or intraoperative findings in 39 patients (40%). In the subset of patients within the superficial and intrafascial group (n = 17), 71% were noted to have PV. In contrast, 4 of the 22 patients (18%) who were believed to have intraperitoneal AASW tracts on the basis of findings on CT did not have PV on diagnostic laparoscopy. The accuracy of CT in assessing the depth of the AASW tract was only 59%.
Results • Overall, the diagnostic performance of CT in detecting intra-abdominal injury was as follows: sensitivity, 96%; specificity, 97%; PPV, 93%; NPV, 99%; and accuracy, 97%. In assisting the practitioner in determining the need for surgical intervention, the diagnostic performance of CT was as follows: sensitivity, 93%; specificity, 93%; PPV, 70%; NPV, 99%; and accuracy, 93%.
hese guidelines apply only to those patients stabbed in the • anteriorabdomen (see anatomic boundaries in box below), who meet • all three of the following criteria: • hemodynamically normal (i.e.. are not hypotensive, tachycardic • or diaphoretic) • have no evidence of peritonitis • have no bowel or omental evisceration through the wound • The presence of any one or more of the above mandates immediate • abdominal exploration - without delay for further investigative • maneuvers or x-rays.
Local Wound Exploration: In stable patients, a stab wound within the boundaries of the anterior abdominal wall (see above) will first be examined for evidence of violation of the anterior abdominal fascia. This procedure is performed under sterile conditions (gown/glove/mask, prepping and draping), using adequate lighting, local anesthesia (1% lidocaine + epi) and instrumentation to extend the margins of the stab wound so as to visually and digitally explore its depth. Cotton-tipped applicators ("Q-tips") are not to be used to probe the wound.
A. If the local wound exploration demonstrates no fascial violation, the wound is irrigated copiously and closed, and the patient may be discharged from the emergency department. Prophylactic antibiotics are not indicated. • B. If the local wound exploration demonstrates violation of the anterior abdominal wall fascia, it should be assumed that the knife entered the peritoneal cavity. The wound is closed in layers after adequate irrigation. The patient will then undergo diagnostic peritoneal lavage (DPL) to determine indications for exploration (see 2. below). Should there be strong contraindications to DPL (multiple prior abdominal operations, ascites, third trimester pregnancy, refusal of procedure by patient), the patient will be observed for a period of no less than 48 hours. Immediate exploration is also an acceptable alternative, after discussion with the patient and the attending trauma surgeon.
I. Diagnostic Peritoneal Lavage: Any of the following "(+) DPL results" mandates abdominal exploration: A. gross blood > 10 ml or any feces or any bile on initial paracentesis • B. RBC count > 50,000 RBC / mm3 • C. WBC count > 500 / mm3 • D. Bacteria, food or vegetable particles on gram stain / microscopic exam
Patients whose DPL results are negative will be admitted for a minimum of 24 hours. During this period of observation they will undergo monitoring of vital signs, frequent abdominal examinations (q 2 hr x 12hrs, then q 4 hr) and repeat CBC at 12 and 24 hours. They will be fed ad lib. Prompt abdominal exploration will be indicated for any patient developing peritoneal irritation, unexplained fever, leukocytosis or hemodynamic instability. Prophylactic antibiotics are not indicated during the observation period. Analgesia will consist of intramuscular NSAIDs while NPO, followed by oral agents once oral intake is tolerated. If none of the abnormalities above are noted after the 24 hour period of observation, the patient may be discharged home under the care of a responsible adult. Follow-up to the Trauma Surgery Clinic should be scheduled for within one week.