Single Ventricle Physiology
Single Ventricle Physiology. Spectrum of Management from Birth to Surgery. Dr. J. Burzynski Division of Pediatric Critical Care University of Iowa. At the end of the talk you should be able to…. Identify group(s) of lesions that function physiologically as single ventricles

Single Ventricle Physiology
E N D
Presentation Transcript
Single Ventricle Physiology Spectrum of Management from Birth to Surgery Dr. J. Burzynski Division of Pediatric Critical Care University of Iowa
At the end of the talk you should be able to… • Identify group(s) of lesions that function physiologically as single ventricles • Identify how these babies present to medical attention • Know key features of pre-operative stabilization and management • Identify the basics of the staged operative approach and post-operative management
3 main ways babies present with congenital heart disease… • SHOCK (obstructed flow to body) • “BLUE”(obstructed or restricted flow to lungs) • HEART FAILURE (excess volume load, ie large AV canal defect) [at least the ones intensivists worry about, innocent murmurs aside…]
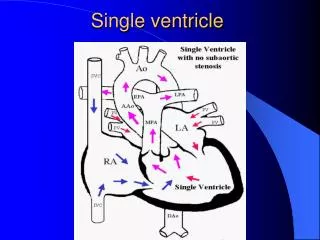
Anatomic variants of the single ventricle: • NOT just hypoplastic left heart syndrome (HLHS) • All generally have mixing of systemic / pulmonary venous return • May also have obstructed venous return
Examples of systemic outflow obstruction… • Classic HLHS (small left-sided structures with aortic atresia) • Critical aortic stenosis/coarctation • Interrupted aortic arch • Mitral valve atresia • Tricuspid atresia (with transposition of great arteries) Among others!
Lesions with obstruction to pulmonary blood flow… • Tricuspid atresia (normal related great arteries) • Pulmonary atresia • Ebstein’s anomaly Again many others!
Spectrum of symptoms based on severity of obstruction • Most of ventricular output directed out the aorta • Anatomic right left shunt at atrial level causing cyanosis
Key feature for presentation and management decisions is: • Presence of outflow obstruction to lungsORbody? (or both) • Is atrial septum open or “restrictive” [Really this is all you need to know!]
The importance of the atrial septum… • Single ventricles must have complete mixing at atrial level • Restrictive defect will cause high CVP (3rd spacing of fluid…) on systemic side • Pulmonary venous hypertension due to high LA pressures can cause significant hypoxemia [Somewhat restrictive ASD can be beneficial however to restrict pulmonary blood flow]
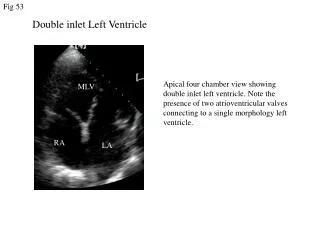
Hypoplastic left heart syndrome (HLHS) 1 - patent foramen ovale 2 - pinched aorta 3 - patent ductus arteriosus 4 - narrowed aorta 5 - hypoplastic left ventricle 6 - aortic atresia Complete mixing at atrial level through PFO
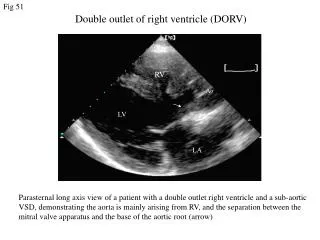
Interrupted aortic arch 1 - interruption of aortic arch 2 - descending aorta connected to pulmonary artery by large patent ductus arteriosus 3 - ventricular septal defect
Systemic outflow obstruction lesions cont’d… • Ductal dependent SYSTEMIC flow • Ventricular outflow to lungs predominantly • R L shunt at ductal level • If no prenatal diagnosis, will present with SHOCK as ductus closes: • Poor perfusion, pulses, metabolic acidosis • Cyanosis due to profound low systemic output • Often accompanying end organ failure (kidney, liver, CNS…)
Keys to adequate resuscitation… • RECOGNITION! • Ductal dependent lesions just as common as sepsis in neonatal shock • ABC’s--usually involves intubation, sedation • Correct metabolic acidosis, usually need fluid boluses +/- inotropy
Resuscitation cont’d… • Prostaglandin infusion! • Any neonate in shock should be started on PG’s • Opens ductus • Improves blood flow in ductal-dependent lesions or inter-circulatory mixing in D-TGA • Dose 0.01-0.1 mcg/kg/min • Side F/X include apnea, vasodilation, fever • If worsening hypoxia think of pulmonary venous obstruction
Resuscitation cont’d… • Aim for oxygen saturation 70-85% (ie not FiO2 = 100%) • Beware of potential for too much pulmonary blood flow (over-circulation) as PVR falls in the first few days • Tolerate “highish” PaCO2 to restrict pulmonary blood flow (ductal-dependent systemic circulation) Transfer to appropriate ICU!
Pre-operative ICU management • Confirm the diagnosis! • Echocardiography (cath rarely needed) • Need to know status of ATRIAL SEPTUM (ASD) • Restrictive ASD leads to profound hypoxemia due to high left atrial pressure, worse outcomes • Evaluation for end organ function (especially if patient presented in shock)
Pre-operative circulatory management Goal is balancing the flow to lungs and body… Fick equations: Qs=VO2 / (CaO2-CmvO2) Qp=VO2 / (CpvO2-CpaO2) VO2= oxygen consumption CaO2=arterial oxygen content = HgB X 1.34 X SpO2 CmvO2=mixed venous oxygen content CpvO2=pulmonary venous oxygen content CpaO2=pulmonary artery oxygen content
Substituting equation for oxygen content equations give: Qp/Qs = (SaO2 - SmvO2) / (SpvO2 - SaO2) Mixed venous oxygen saturation Pulmonary venous saturation [Assuming that SpvO2 = 95% (probably close to true in pre-op but NOT post-op care]
Key here is that systemic saturation may be misleading • SVO2 may drop, with more blood flow to lungs thereby preserving SaO2 • Mixed venous saturation useful in pre-op infants to help treatment decisions • Follow serum lactate for signs of anaerobic metabolism • Keeping Qp/Qs <1.5:1 is goal • Flow largely dependent on resistance of each (systemic and pulmonary)
Managing Qp • With ductal-dependent systemic circulation, large amounts of Qp usually (ventricular output predominantly to lungs) • As Qp/Qs approaches 2, volume overload/CHF develops • Want to minimize pulmonary blood flow / maximize systemic flow and oxygen delivery
Therapeutic interventions… • Minimize FiO2----21%; may blend w/ N2 to deliver FiO2 16-18% • Alveolar hypoxia will elevate PVR • Beware that prolonged sub-atmospheric O2 may lead to sustained elevated PVR • Hypoventilation • PVR sensitive to pH • May need mechanical ventilation, sedation +/- paralysis • Addition of inspired CO2 also used in some centres (unlike N2 - may improve DO2)
If mechanically ventilated, increasing PEEP above the FRC (functional residual capacity) will raise PVR • Tension on intra-alveolar arterioles
The systemic circulation… • Promoting systemic flow by dropping SVR • Goal is to maximize DO2 (oxygen delivery) • Pharmacotherapy usual route • No universal therapy • Afterload reducing agents such as Milrinone, Nitroprusside, Phenoxybenzamine are commonly used • Sedation/paralysis will decrease VO2 (oxygen utilization)
Other systems… • Beware of enteral feeds due to risks of gut ischemia/bacterial translocation in ductal-dependent systemic flow • Intestinal blood flow also has typically low PaO2 in cyanotic lesions as well • Renal function usually recoverable after initial “hit”
Surgical management… • Timing is institution-dependent, but is generally performed in the 1st week of life • Medical management alone sometimes cannot “balance” circulations adequately, leading to surgery • Goal is to create unobstructed venous return (systemic/pulmonary) and systemic blood flow • Need controlled source of Qp
Options: • Classic Norwood operation: • Blalock-Taussig shunt 3.5 or 4 mm graft from innominate or subclavian artery to pulmonary artery • Arch augmentation (different techniques) • Atrial septectomy
Sano modification: • Arch augmentation • Right ventricle to PA conduit (5 mm usually, dependent on size) • Described initially by Norwood but abandoned (large shunts used) • Resurrected in Japan by Sano
Sano shunt with augmented aortic arch Beginning of arch augmentation
Sano modification cont’d… • Published data: showing less need for “ICU care” to manipulate circulatory balance • Seems less prone to sudden circulatory collapse
Hybrid procedures… • Recent description of PA banding with ductal stenting in neonatal period • Used in some centres as bridge to transplant • Others use as “1st stage” with arch reconstruction + cavopulmonary anastomosis at 3-6 months
Numbers small however • Anecdotal evidence that ductal stent has potential to make arch repair very difficult • Unclear where this will end up as an option
Post-operative management… General principles: • Similar to pre-op management of circulation in series with addition of the effects of CPB on PVR/myocardium • Emphasis has been on balancing PVR/ SVR with respiratory or pharmacologic management
Post-operative management cont’d… • Emphasis on central venous oxygen saturation to estimate adequacy of O2 delivery • Centres use either indwelling oximetric catheter or intermittent blood gas monitoring • Remember that difference between arterial and mixed venous saturation is more indicative of overall oxygen delivery (A-V O2 difference)
Summary… • Just like all congenital heart disease: need to know where the blood goes/flows • Counter-intuitive to think of low SpO2 as being better… • Draw it out if need be!