Download
1 / 17
280 likes | 976 Vues
LIPID METABOLISM IN THYROID DISEASE. John MF Adam. Diabetes and Lipid Centre, Dr. Wahidin Sudirohusodo Hospital Division of Endocrinology and Metabolism, Department of Internal Medicine, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia. INTRODUCTION.

E N D
LIPID METABOLISM IN THYROID DISEASE John MF Adam Diabetes and Lipid Centre, Dr. WahidinSudirohusodo Hospital Division of Endocrinology and Metabolism, Department of Internal Medicine, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
INTRODUCTION It is well known that alteration in thyroid hormones, results in changes in the composition of lipid profiles These changes in lipid profiles can occur in subjects with hyperthyroidism as well as hypothyroidism, subclinical as well as overt classical cases Clinically, lipid changes are more frequently seen in subjects with hypothyroidism
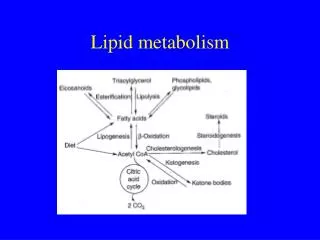
LIPOPROTEIN METABOLISM Endogenous pathway (from the liver) Exogenous pathway (from food intake)
LIPOPROTEIN METABOLISM Liver VLDL IDL LDL VLDL Macrophage HDL Endogenous pathway Fat cells FFA RCTP remnants cholesterol Exogenous pathway chylomicron cholesterol RCTP = reverse cholesterol transport pathway stools intestine Food Shepherd J. Eur Heart J Supplements 2001;3(suppl E):E2-E5
IDL LDL LIPOPROTEIN METABOLISM – endogenous pathway Liver LDL receptor Scavenger receptor-A / CD 36 VLDL VLDL ABC-1 VLDL SRB-1 CE CE Macrophage CE Ox- LDL CETP Cholesterol TG CETP = cholesterol ester transport protein LCAT=lecithin:cholesterol acyltransferase LCAT HDL Nascent HDL Kwiterovich PO, Jr. The metabolic pathways of high-density lipoprotein, low-density lipoprotein, and triglycerides: A current review. Am J Cardiol 2000;86:5L-10L
T4 The way thyroid hormones modulate lipid metabolism by variety of ways-hyperthyroidism + 3 LPL VLDL IDL + 2 T4 CETP CETP HDL2 LPL HL T4 + HL T4 4 + 4 HDL3 CETP 5 Liver - Ox-LDL LDL LDL Receptor LDL Receptor + Peripheral tissue Macrophage T4 1 Liberopoulos EN. Hormones 2002, 1(14): 218-223
DYSLIPIDEMIA - HYPERTHYROIDISM Decrease in total-cholesterol, LDL-cholesterol, apolipoproteinB, HDL-cholesterol, TG levels remain unchanged
T4 The way thyroid hormones modulate lipid metabolism by variety of ways-hypothyroidism - 3 LPL VLDL IDL - 2 T4 CETP CETP HDL2 LPL HL T4 4 - HL T4 - 4 HDL3 CETP 5 Liver + Ox-LDL LDL LDL Receptor LDL Receptor - Peripheral tissue Macrophage T4 1 Liberopoulos EN. Hormones 2002, 1(14): 218-223
DYSLIPIDEMIA – HYPOTHYROIDISM Raised of total-cholesterol, LDL-cholesterol, Ox-LDL-cholesterol, hyper TG, HDL-cholesterol, increased Lp (a) Clinically, lipid changes are more frequently seen in subjects with hypothyroidism These abnormal dyslipidemia enhanced the risk of CAD
HYPOTHYROIDISM In general population (western countries) hypothyroidism is more frequent than hyperthyroidism (9.5% vs 2.2% ) More frequent in the western countries due to: - high incidence of autoimmune thyroiditis Hashimoto - active screening among elderly subjects - more frequent use of I131 for Graves’ hyperthyroidism Indonesia very low: - low prevalence of Hashimoto thyroiditis, our observa- tional study 2000 – 2010 only 45 patients - screening in the elderly is not a routine procedure - less frequent use I131 for Graves’ hyperthyroidism
THE MANAGEMENT OF DYSLIPIDEMIA IN THYROID DISEASE Levels of total-C and LDL-C tend to increase as the thyroid function declines. Hypothyroidism constitutes a significant cause of secondary dyslipidemia Therefore the treatment of thyroid dyslipidemia is always focus on hypothyroidism Substitution with L-thyroxine therapy significantly improves the abnormal dyslipidemia, especially in overt hypothyroidism The reduction of cholesterol was larger in individuals with higher cholesterol levels
MANAGEMENT OF DYSLIPIDEMIA IN SUBCLINICAL HYPOTHYROIDISM Subclinical hypothyroidism (SH) is defined by mildly elevated TSH levels (up to 10 uIU/L) with normal levels of FT4 and FT3 SH been detected with increasing frequency in recent years (more common than overt hypothyroidism) and causing major controversies concerning management and treating with L-thyroxin SH patients, tend to have high levels of total-C and LDL-C, ApoB and LP(a)
MANAGEMENT OF DYSLIPIDEMIA IN SUBCLINICAL HYPOTHYROIDISM This dyslipidemia, make SH has been associated with in- creased risk of CAD Even though, the treatment with L-thyroxine is still contro-versies Monzani F et al: L-T4 replacement therapy improved the atherogenic lipoprotein profiles and CIMT thickening Carracio N et al: L-T4 treatment has significant decrease of both total-C and LDL-C Hueston WJ et al: SH does not appear to be associated with abnormal serum lipid Pearca EN: Clinical trials to date have not shown a beneficial effect of L- thyroxine on serum lid profiles in SH
CASE TE male, 32 years, no DM, not HT, but heavy smoker, was diagnosis with thyroid follicular Ca. A total thyroidecto-my was performed followed by I131. Thyrax suppres-sion was given but sub-optimal (1992) The cholesterol levels was always high (250-325 mg/dL), and still smoking, while TSHs showed subclinical hypothyridism In February 1998, he was admitted to the hospital due to acute myocardial infarction AMI due to dyslipidemia in subclinical hypothyroidism ??
MANAGEMENT OF DYSLIPIDEMIA IN THYROID DISEASESUMMARY Dyslipidemia is frequent in hypothyroidism Substitution with L-thyroxin will improve the abnormal lipid profiles L-thyroxin for subclinical hypothyroidism remain contro-versial Since both overt and subclinical hypothyroidism may occur in elderly subjects, where either diabetes mellitus, hyper-tension or CVD may coincidence with these conditions, statin therapy should be consider for the prevention of CVD
THANK YOU Thank you AOTA Bali, 22-24 Oktober 2012