Download
1 / 22
220 likes | 255 Vues
Explore the goals and techniques of hip arthroscopy for joint preservation, diagnosis, and treatment of hip pathologies. Learn about hip preservation, diagnosis methods, labral tears, FAI, and postoperative rehabilitation phases for optimal outcomes.

E N D
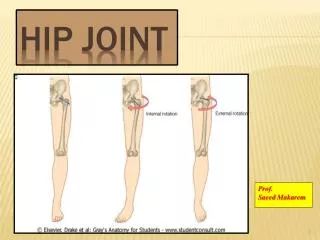
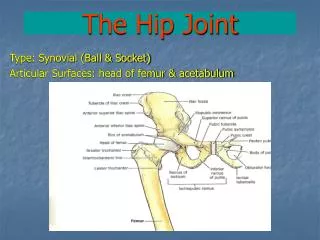
Hip Arthroscopy and Physical Therapy in Joint Preservation • Daniel S. Lamar M.D.
Hip Arthroscopy- Goals • Relieve Pain • Improve function • Improve Longevity???
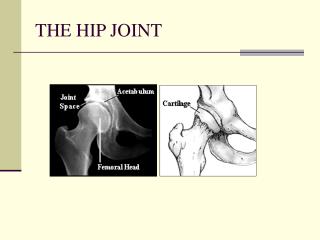
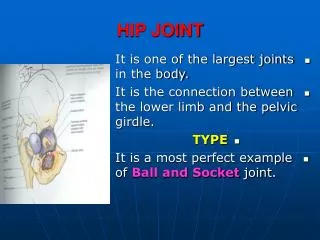
Hip Preservation • Central premise- Improve the mechanical issues that predispose the joint to developing arthritis • Essentially need to change the mechanics of the ball and socket in order to reduce continued injury
Factors associated with Pathologic Mechanics • Dynamic • loss of offset and sphericity at HN junction (CAM) • Acetabular overcoverage, focal or global (Pincer) • Instability, posterior subluxation • Static • acetabular undercoverage (dysplasia)
Hip Pathology and Treatment • CAM lesion- remove bump/ improve sphericity • Pincer lesion- Rim trimming vs femoral osteoplasty • Labral Tear- Repair vs debride vs reconstruct • Instability- Capsular plication vs PAO • Dysplasia- Debride vs PAO • Arthritis- Symptomatic relief/debride vs THA • Cartilage defects- Microfracture, OATS, Rim trim
Diagnosis • Make the correct diagnosis! • Ensure that the hip is the source of pain • H+P (C sign) • Diagnostic injection • Then ID which structure/issue within the hip is the culprit and its source of origination
Diagnosis • MRI can under appreciate severity of cartilage injury • MRA is better, but not perfect- great at demonstrating magnitude of labral pathology • CT scan with 3D recon is a great preop tool
Labral Tear • Most common source of pain in non-arthritic hips • Associated with FAI 87% of the time (Wenger CORR 2004)
FAI • CAM Pincer
CAM/Pistol Grip • Overstuffing of anterolateral joint • Younger, athletic males • Short fem neck, SCFE • Usually see cartilage delamination with labral tear • Femoral cartilage usually spared until late
Pincer • Pincer • tends to spare cartilage early • contra coup post cartilage wear • herniation pits femoral neck • local overgrowth vs global protrusio vs acetabular retroversion
Treatment- Hip Preservation • Involves correctly identifying injury pattern • Removing bony overgrowth (3D CT scan) • Repairing labrum vs debride -suggestion that restoring the seal by repairing labrum if at all possible can decrease degenerative progression Larsen, Am J Sports Med 2012. • Treating established cartilage injury
Outcomes • Gupta, Am J Sports Med. 2015, 2yr f/u results on primary hip arthroscopy • 595 pts • Improved HHS 61.29-82.02 • 7.7% revision scope, 9.2% conversion to THA • Linder, Arthroscopy. 2015, 2 yr f/u outcome on age-matched controls • Ave age 20.3 vs 54.8 • HHS 62.9-84.2 vs 61.2-82.2 • Survivorship 98% vs 82.7%
Outcomes • Domb, Arthroscopy 2015, How much arthritis is too much? • reviewed 518 articles, 15 included,2,051 hips, age 40.2 • 1,195 had some sign of cartilage damage • 345 converted to THA (duration of f/u)
Postop Rehab- Phase 1 0-3 weeks • Protect repair • Reduce pain • Avoid muscular inhibition • Foot down WB x 2 weeks • ROM limitations • ext-flex 0-90 degrees • IR- 0, ER 20-30 • Exercises • Isometrics, bike no resist,
Phase 2 • 3-6 weeks • Goals • Protect repair • Restore FROM • Normalize gait • Begin strengthening • Balance progression • No forced stretching so avoid stress to repair
Phase 3 • 6-10 weeks • Goals • Full hip ROM • Normal gait • Strengthening continued with emphasis on glut med • Step and squat progression
Phase 4 • 10-12 weeks • Goals • Restore full muscle strength and endurance • Restore cardio • No contact activity • Avoid mobs and aggressive stretch
Phase 5 • 12+ weeks • Sport specific training • Agility • Advance back to activities as tolerated
Take Away Points • Making the correct diagnosis is not always easy, but critical • Our understanding of hip kinematics and the mechanics of pathologic progression has improved dramatically • Instrumentation and surgical technique are allowing us to tx and hopefully prevent more pathology than ever • The literature regarding disease progression and the effects of arthroscopy to modify that course is growing, but in its infancy.
Take Away Points • Hip arthroscopist less excited about surgery with existing arthritis at any age • Hip Arthroscopy has excellent outcomes in the well selected patient • THA has excellent results, and seem to be improving in younger patients