Download
1 / 50
580 likes | 1.09k Vues
Functional Use of Kinesio® Taping After a Brain Injury. Presented By: Christina Jelenik OTR/L, CKTP Danielle Dreyfus PT, CKTP Barbara J. Stygles OTR/L, CKTP, CBIS. Disclaimer .

E N D
Functional Use of Kinesio® Taping After a Brain Injury Presented By: Christina Jelenik OTR/L, CKTP Danielle Dreyfus PT, CKTP Barbara J. Stygles OTR/L, CKTP, CBIS
Disclaimer This information release is the property of NERH hospital. It may not be modified, sold for profit or used in commercial documents. The information is provided “as is” without any expressed or implied warranty. While all information in this document is believed to be correct at the time of writing, this document is for educational purposes only and does not purport to provide legal advice. The identification of an organization or product in this information does not imply any form of endorsement. Attendance of this lecture does not provide any individual or clinician the capability to use the Kinesio® taping method or it’s insignia. Clinicians and individuals must consult a physician and a CKTP if they believe a patient is appropriate to use this modality.
Outline • Kinesio® Tex Tape vs. McConnell tape vs. athletic tape • Qualities • Five main physiological effects • Diagnostic indicators • Contraindications/Precautions • Evaluation • Application • Removal
Kinesio® Tape • “The Kinesio® Taping Method is designed to facilitate the body’s natural healing process while allowing support and stability to muscles and joints without restricting the body’s range of motion. It is used to successfully treat a variety of orthopedic, neuromuscular, neurological and medical conditions. Both Kinesio® Tex Tape and the training protocol have shown results that would have been unheard of using older methods and materials.” • Founded by Dr. Kenzo Kase • Invented in 1973 in Japan • Can be used in conjunction with other modalities
Kinesio® Tex Tape vs. McConnell tape vs. Athletic Tape • Athletic Tape • Acute injuries and injury prevention • Requires pre-tape or spray adhesive • Compression of skin joint and muscle • Limits Motion • Contains latex • McConnell Taping • Bracing or strapping • Extremely rigid cotton mesh tape • Requires pre-tape • Poor adhesive quality when wet • Primarily orthopedic usage • Limited wear time
Qualities of Kinesio® Taping • Stretches along a longitudinal axis only • Thickness and weight is similar to skin • 100% medical grade, acrylic, heat activated adhesive • No medicinal properties in tape • Latex-free • Can be worn 3-5 days • Water resistant • Breathable
Qualities of Kinesio® Taping • Safe for pediatrics and geriatrics • Allows for normal ROM • Restores epidermal tissue homeostasis • More economical • Easy to apply • Allows for treatment between taping • Enhances muscular, joint and circulatory function
Five Main Physiological Effects • Skin • Scar management • Fascia • Fasciitis • Compartment syndromes • ITB • Lateral epicondylitis • Joint • Functional correction • Mechanical correction
Five Main Physiological Effects • Circulatory-Lymphatic • Edema • Hematomas/Bruising • Muscle • Inhibition • Facilitation
Diagnostic Indicators • Decreased muscle strength • Facilitation • Positional holding • Spring assistance • Increased tone and overactive muscles • Inhibition • Swelling • Pain • Scar Tissues • Asymmetrical posture/movement • Sensory Stimulation • Hypermobility
Contraindications • Active malignancy site • Active cellulitis or skin infections • Can not be used over open wounds • DVT
Precautions • Diabetes • Kidney Disease • Liver Disease or any organ that assists with fluid removal • CHF • CAD or Bruits in the carotid artery • Fragile or healing skin • Sunburn, irradiated skin, • History of tape allergy • Lymphoedema • Respiratory Conditions • Pregnancy • Allergies • Strawberry, kiwi, bananas • Hypersensitivity
I Cut Y Cut X Cut Fan Cut Web Cut Button Hole Cut 13
“I” Cut • Easy • Common • Localized treatment • High stimuli • Usually one tissue
“Y” Cut • Broad treatment area • Treatment occurs at the tape ends and between the tape • Lower Stimuli • Allows treatment of two different structures
“X” Cut • Moderate Stimuli • Focus of treatment is in the middle of the tape • Dissipates tension faster • Good for muscles with numerous attachments (biceps) • Works well for muscles that have a broad origin and insertion (quadratuslumborum)
“Donut Hole” Cut • Used over areas with boney prominences • Used for painful, edematous areas • Used to avoid wounds, broken skin, or incisions • “Button Hole” Cut • Used over hand and/or foot
“Fan” Cut • Broadest area of treatment • Least amount of stimulus • Good for fingers and toes • Good for edema management
“Web” Cut • Effective for large area edema resolution, space
What is the tension? Distal to proximal (insertion to origin) • To inhibit overused muscles, acute conditions, muscle spasms • 15%-25% tension Proximal to Distal (origin to insertion) • To facilitate weak muscle-chronic conditions, rehabilitation • 15%-50% The recoil of the tape is what provides the therapy Tensions greater than 50% are for corrective techniques only
What is the orientation? • Distal to proximal (insertion to origin) inhibits over used muscles • Muscle spasms • Acute conditions • Proximal to distal (origin to insertion) facilitates weak muscles • Rehabilitation • Chronic conditions
Top portion filled out by primary therapist, bottom half to be filled out my therapist applying tape Name________________________________ Room #________________ Dx: ______________________________________________________________ PMH:_____________________________________________________________ Primary therapist: ________________________________________________ Does the patient have any of the following? Check all that applyMalignancy Allergy: Strawberry, kiwi, banana, tape Fragile or Healing Skin Diabetes Cellulitis or healing skin Kidney Disease Open wounds Lymphodema DVT Respiratory Conditions Previous skin reaction to this product CHF Infections CAD or Bruitis in the carotid artery Irradiated skin Pregnancy Areas to be addressed:____________________________________________________ To be filled out by therapist applying the tape Assessment: Treatment Area: Skin, Circulatory/lymphatic, Fascia, Muscle, Joint, Ligament, Specify location:____________________________________________________ Purpose of Tape: Facilitation, Inhibition, edema control, pain control Type of cut:________________________________________ Direction of tape: ___________________________________ Length: ___________________________________________ Tension:___________________________________________ Date Applied:_______________________________________ Results:_____________________________________________ Applied by:____________________________________ Education sheets given to pt, nursing, and posted in room
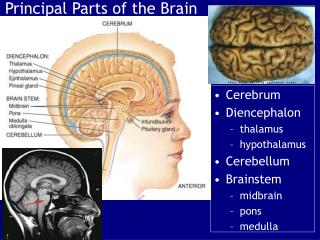
Common Deficits After A Brain Injury • Changes in muscle tone • Changes in strength • Pain • Swelling • Postural Changes • Secondary Injuries • Bruising, fractures, etc.
Secondary Injuries • Hematoma/ Bruising • Ligament injury • Pain • Surgical site, strained muscle, whiplash • Swelling • Orthopedic injury
What is the treatment area? • Muscle • Joint • Ligament • Fascia • Skin • Circulatory
What is the reason for taping? • Tonal changes • Decreased strength • Muscle overuse • Edema • Postural changes • Pain • Bruising
Changes in Muscle Tone • Hypertonicity • Tape for inhibition • Increase passive range of motion • Decrease pain • Allow for increased active range of motion
Decreased Strength • Tape for facilitation • Stabilize joints • Promote active range of motion
Muscle Overuse • Tape for inhibition • Decrease pain • Increase active ROM within a normal range
Edema • Tape is positioned to recoil and promote drainage towards a patent, healthy lymph node
Postural Changes • Why are there postural changes? • Weak muscles • Overactive muscles (spasm) • Increased tone • Decreased tone
Pain • What is the cause? • Swelling? • Tightness? • Tone? • Positioning? • Hematoma?
Bruising • Tape to improve drainage of stagnant blood to dissipate bruising
What is the Cut? I Cut Y Cut X Cut Fan Cut Web Cut Button Hole Cut 36
What is the orientation? • Distal to proximal (insertion to origin) inhibits over used muscles • Muscle spasms • Acute conditions • Proximal to distal (origin to insertion) facilitates weak muscles • Rehabilitation • Chronic conditions 38
Application Process • Assess • Tape • Re-assess
Kinesio® Tex Tape Removal Instructions • Tape will be removed by therapist except in case of emergency or unexpected discharge • Kinesio® Tex Tape can be kept on a pt. for up to five days if a pt. reports any increased pain, swelling, or uncontrolled itching please remove tape in the following manner. If you do not follow these instructions the pt.’s skin may be damaged. • Massage tape thoroughly with lotion (this will break down the adhesive.) • Slowly peel away the tape starting at a corner • As you slowly peel provide tension to skin, this will decrease pain. • Once the tape is removed, examine skin and clean thoroughly .
Please do not remove blue/pink/black Tape from patient’s______________________ Thank You, If you have any questions please contact _________________ ext._________
Case Study #1 • 62year old male • Diagnosis • Lyme Meningitis • Admitted to acute rehabilitation 8/12/11 • Admit FIM • Eating: 5 • Grooming: 5 • Ambulation: 5 (160 feet with a rolling walker) • Bathing : 4 • Upper Body Dressing: 4 • Lower Body Dressing:4 • Toileting: 4 • Toilet Transfer: 4 • Transfers 4 • Complaints • Bilateral shoulder pain • Complained of pain as “band-like squeezing” around upper thorax and feeling like “pulls him forward” • Limited sitting tolerance • Weakness • Poor posture with all mobility resulting in decreased dynamic balance • Bilateral scapular winging
Results Case Study #1 • Discharged from acute rehabilitation on 8/24/11 • Discharge FIM • Eating: 7 • Grooming: 7 • Ambulation: 7 (greater than 1000 feet without an assistive device) • Bathing: 7 • Upper Body Dressing: 7 • Lower Body Dressing:7 • Toileting: 7 • Toilet Transfer: 7 • Transfers: 7 • FIM Change: 28 • LOS Efficiency: 2.15 • Clinical observations • Improved posture, increased sitting tolerance, increased dynamic balance (no longer required device when ambulating) • Patient Observations • Decrease pain, increased functional ability to use upper extremities, increased sitting tolerance
Case Study #2 • 52 year old right handed Caucasian male • Diagnosis • Left MCA CVA • Admitted to acute rehabilitation 9/8/11 • Admit FIM • Eating: 5 • Grooming: 3 • Bathing: 1 • Upper Body Dressing: 1 • Lower Body Dressing: 1 • Toileting: 4 • Toiler Transfer: 2 • Bed to Wheelchair Transfer: 2 • Ambulation: 1 • Complaints • Weakness of right upper and lower extremities • Decreased independence with ADLs and mobility
Results Case Study #2 • Discharged from acute rehabilitation: 10/11/11 • Discharge FIM • Eating: 6 • Grooming: 7 • Bathing: 7 • Upper Body Dressing: 7 • Lower Body Dressing: 7 • Toileting: 7 • Toiler Transfer: 7 • Bed to Wheelchair Transfer: 6 • Ambulation: 6 • FIM Change: 55 • LOS Efficiency: 3 • Clinical observations • Dramatic functional improvements • Patient Observations • Increased independence in performing all activities of daily living, not feeling like a burden to his teenage children
Tape Demonstration • Facilitation of External Rotation • Finger extension with a functional correction of the wrist • Inhibition of the IT Band results
Disclaimer This information release is the property of NERH hospital. It may not be modified, sold for profit or used in commercial documents. The information is provided “as is” without any expressed or implied warranty. While all information in this document is believed to be correct at the time of writing, this document is for educational purposes only and does not purport to provide legal advice. The identification of an organization or product in this information does not imply any form of endorsement. Attendance of this lecture does not provide any individual or clinician the capability to use the Kinesio® taping method or it’s insignia. Clinicians and individuals must consult a physician and a CKTP if they believe a patient is appropriate to use this modality.