Download
1 / 136
1.36k likes | 1.44k Vues
Explore the pathophysiology, assessment, and management of CNS emergencies, including structural and circulatory changes often due to trauma. Learn about altered mental states and coma, as well as the importance of ABCs in assessing and managing patients. Discover causes of altered mental status and the mainstays of therapy for various conditions. Dive into cerebrovascular accidents, their pathophysiology, risk factors, and classification. Gain insights into differentiating AMS causes and essential interventions for optimal patient care.

E N D
CNS Disorders EMS Professions Temple College
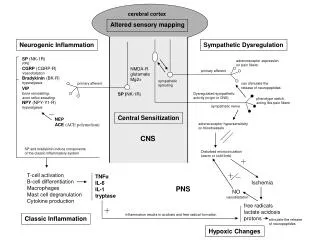
Pathophysiology of CNS Emergencies • Structural Changes • Often due to Trauma but not always • Circulatory Changes • Inadequate Perfusion • Alterations of ICP • Response to insult • Toxic Metabolic states • Alteration to blood chemistry or introduction of toxins • Psychiatric ‘mimicking’
ICP Review • CBF is a factor of CPP & CVR • If CPP , then CBF • If CVR , then CBF most likely • CPP = MAP - ICP • MAP = Diastolic + 1/3 PP • PP = SBP - DBP • PCO2 has greatest effect on CVR • Sympathomimetics may CVR
ICP Review • As PCO2, CVR • Therefore, if PCO2, CVR • Then, as CVR , CBF • Normal ICP < 15 mm Hg • As ICP , CPP then CBF • Compensation for ICP via MAP • Cushing’s Reflex (Triad) • Cushing’s triad with coma indicates possible herniation
Coma • A decreased state of consciousness from which a patient cannot be aroused • Mechanisms • Structural lesions • Toxic Metabolic states • Psychiatric ‘mimicking’
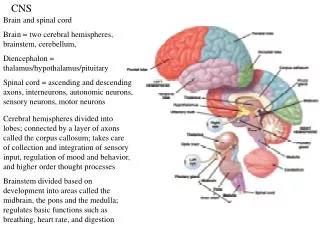
Brain injury Recall that Brain injury is often shown by: Altered Mental Status Seizures Localizing signs
Is unconsciousness itself an immediate life threat? Loss of airway Vomiting, aspiration YES, IT IS!
Altered Mental State Manage ABC’s Before Investigating Cause!
Initial Assessment/Management Airway Open, clear, maintain If trauma or + history, control C-spine Breathing Presence? Adequacy (rate, tidal volume)? High concentration O2 on ALL patients with altered mental status Assist ventilations prn Circulation Pulses? Adequate Perfusion?
Investigate Cause DERM D = Depth of Coma E = Eyes R = Respiratory Pattern M = Motor Function
D = Depth of Coma What does patient respond to? How does he respond? Avoid use of non-specific terms like “stuporous”, “semi-conscious”, “lethargic”, “obtunded”
D = Depth of Coma AVPU Glasgow Scale (later) Describe level of consciousness in terms of reproducible findings
E = Eyes Pupils Size - mid, dilated or constricted measurement - e.g. 4 mm Shape - round, oval, pontine Equality - equal in size Symmetry - equal in reaction/response Response to light Yes or No How?
R = Respiratory Pattern Depth Unusually deep or shallow? Pattern Regular or Unusual pattern Can you identify the pattern?
M = Motor Function Paralysis? Where? Muscle tone? Rigid or Flaccid Movement? Where? What is it like? Posturing? How? Symmetrical Motor Function?
Physical Exam Vital Signs Shock? Increased ICP? Hypoxia/Hypercarbia Diagnostics Dysrhythmias? Blood glucose Oxygen saturation
Physical Exam Detailed (Head-to-Toe) Exam Injuries causing coma? Injuries caused by coma? Clues to the cause
Probable Causes of AMS Not enough Oxygen Not enough Sugar Not enough blood flow to deliver oxygen, sugar Direct brain injury Structural Metabolic
Structural Asymmetrical deficits Unequal pupils Afebrile History of trauma, structural abnormality Often a rapid onset Metabolic Symmetrical deficits Equal pupils (? altered function) ? Fever History of metabolic disorder or illness Rapid onset less likely Differentiating AMS Causes
Management • Maintain ABCs • Attempt to identify cause • Mainstays of therapy • Oxygenation/Ventilation • IV fluids appropriate for the patient • D50 (if hypoglycemic) • Narcan if possibility of opiate OD • Flumazenil in known benzo only OD
Alcohol Epilepsy Insulin Overdose Uremia (Metabolic causes) Trauma Infection Psychogenic Stroke/Syncope AEIOU TIPS
Cerebrovascular Accident • Any disease process that disrupts blood flow to a distinct region of the brain • Transient Ischemic Attack (TIA) • S/S less than 24 hours without permanent neuro deficits
Cerebrovascular Accident • 500,000/yr in US • 25% die • Survivors often socially, financially devastated • $20 billion in medical costs, lost wages
Cerebrovascular Accident (CVA) • Pathophysiology • Thrombosis (brain itself) • Embolus (head, neck or heart) • Hemorrhage (within brain) • Ischemia (systemic blood flow)
Hypertension Cigarette smoking Diabetes Mellitus Heart disease Hyperlipidemia Cardiovascular disease Chronic atrial fibrillation Sickle cell disease Polycythemia Hypercoagulability Birth control pill use Cocaine use Predisposing Factors: Modifiable
Age Gender Race Prior stroke Heredity Predisposing Factors: Unmodifiable
CVA Mechanisms • Ischemic stroke--80 to 85% • Hemorrhagic stroke--15 to 20%
Thrombus Embolus Aneurysm Arrhythmia Hypovolemia CVA Origin
Ischemic Stroke • Blood vessel occlusion • Thrombosis • Embolism • Plaque fragments from carotids • Chronic atrial fibrillation • Fat particles • IV substance abuse particulates • Systemic hypoperfusion • Pump failure • Hypovolemia
Ischemic Stroke Syndromes • Transient Ischemic Attack (TIA) • Neurological deficits that resolve in 24 hours or less (most in 30 minutes) • Commonly result from carotid artery disease • Same symptoms as CVA • Often warning sign of impeding CVA • 5% risk of stroke per year
Ischemic Stroke Syndromes • Dominant Hemisphere Infarction • Contralateral weakness, numbness • Contralateral blurring of vision of half the visual field in both eyes • Difficulty pronouncing words (dysarthria) • Difficulty speaking or understanding speech (dysphasia or aphasia)
Ischemic Stroke Syndromes • Nondominant Hemisphere Infarction • Contralateral weakness, numbness • Contralateral visual field cut • Neglect of contralateral extremities • Constructional apraxia (difficulty drawing figures like a clock face) • Dysarthria • Usually NOT dysphasic or aphasic
Ischemic Stroke Syndromes • Vertebrobasilar Syndrome • Involves blood flow to brainstem, cerebellum, and visual cortex • Dizziness, vertigo • Diplopia • Dysphagia • Ataxia, bilateral limb weakness
Hemorrhagic Stroke • 30 to 50% 30-day mortality • Younger patient population • Two subtypes: • Intracerebral, usually 2o to hypertension • Subarachnoid, usually from berry aneurysms
Hemorrhagic Stroke Syndromes • Intracerebral Hemorrhage • Headache, nausea, vomiting precede deficits • Patients commonly have decreased LOC with extreme hypertension • Contralateral hemiplegia, hemianesthesia • Possible aphasia, extremity neglect depending on hemisphere involved
Hemorrhagic Stroke Syndromes • Subarachnoid Hemorrhage
CVA Assessment • Presentation of CVA varies with area(s) of brain involved and type of CVA
CVA Presentation • Brain can show injury in only three ways: • Decreased LOC • Seizures • Localizing signs • Hemiparesis or hemiplegia • Dysphasia (Receptive or expressive) • Visual disturbances • Gait disturbances • Inappropriate affect • Bizarre behavior • Incontinence
Cincinnati Prehospital Stroke Scale • Have patient smile (“Facial Droop”) • Normal: Both sides of face move equally well • Abnormal: One side does not move as well as other • Have patient close eyes and hold arms out (“Arm Drift”) • Normal: Both arms drift same amount or do not drift • Abnormal: One arm does not drift or one drifts down compared to other or can’t move arms • Have patient say, “You can’t teach an old dog new tricks.” (“Speech”) • Normal: Correct words, no slurring • Abnormal: Slurs words, uses inappropriate words, or unable to speak
Assessment • Signs & Symptoms • Ischemic S&S usually of slower onset • Hemiparesis or hemiplegia • Numbness or decreased sensation of face or unilateral • Altered LOC or coma • Convulsions • Visual disturbances • Slurred or inappropriate speech • Headache or dizziness
Assessment • Signs & Symptoms • Cerebral Embolus with rapid onset • Emboli from valvular HD or Afib • rapid onset • Often with an identifiable cause (e.g. Afib, Valvular heart disease, recent long bone fracture)
Assessment • Signs & Symptoms • Cerebral hemorrhage associated with rapid onset • high mortality rate • Often with severe HA (“Worst headache ever”) • N/V • Rapid decrease in LOC or seizure • Coma, Cushing’s and Herniation
Assessment • History • Associated Altered LOC or Seizure? • Onset/Precipitating factors? • Initial symptoms and progression? • Dizziness, Severe HA, N/V • Previous CVA or TIA? • Previous neuro deficits? • Concomitant illnesses? • Sickle Cell Disease • Atrial fibrillation • Risk factors for stroke & thrombus formation? • BCP, Smoking • HTN, CVD
Physical Exam Mental Status & Behavior Extremity Motor & Sensory Gait Pupils & Vision Cincinnati Prehospital Stroke Scale Evidence of Cushing’s or Herniation Blood glucose level Assessment
CVA Management Basic Objective Improve cerebral blood flow and oxygenation
CVA Management • Airway • If no gag reflex, intubate • Otherwise, position to ensure drainage of secretions • Suction prn • Breathing • Oxygen via NRB • Ventilate with BVM and O2 if rate or tidal volume inadequate • Intubate if herniating
CVA Management • Controlled hyperventilation if intracranial hemorrhage suspected with increased ICP and neurologic deterioration • Indicators • Sudden onset • Headache • Rapid loss of consciousness • Seizures • Unequal pupils
CVA Management • Circulation • Check blood glucose level • Hypoglycemia may mimic CVA • Treat hypoglycemia with D50 • Establish IV Access • Draw blood samples • TKO • avoid solutions with glucose • Monitor ECG • 10% of CVAs are associated with cardiac event • 12 Lead ECG if suspected ischemia