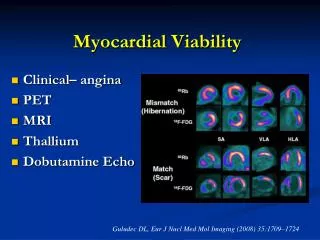
Myocardial Viability
A major teaching hospital of Harvard Medical School. Myocardial Viability. Thomas H. Hauser MD, MMSc, MPH, FACC Director of Nuclear Cardiology Beth Israel Deaconess Medical Center Instructor in Medicine Harvard Medical School Boston, MA. Outline. SPECT PET CMR. Imaging Protocol.

Myocardial Viability
E N D
Presentation Transcript
A major teaching hospital of Harvard Medical School Myocardial Viability Thomas H. Hauser MD, MMSc, MPH, FACC Director of Nuclear Cardiology Beth Israel Deaconess Medical Center Instructor in Medicine Harvard Medical School Boston, MA
Outline • SPECT • PET • CMR
Imaging Protocol • Stress: Prone 99mTc-Sestamibi • Rest: Prone 201Tl
Case 1 Rest Stress
Clinical Data • 58 year-old man with diabetes, hypertension, chronic renal insufficiency, tobacco use, prior heroin abuse and liver transplantation two years ago due to hepatitides B and C. • One week prior to admission he was admitted to another hospital with community acquired pneumonia. He was discharged two days prior to admission. • He presented on the day of admission with chest pain for 12 hours. In the ER he was noted to have anterior ST elevation.
Clinical Data • He was referred for surgical revascularization. The surgical team requested evaluation of myocardial viability given his delayed presentation and the concern for limited myocardial salvage.
Stress Protocol • Dobutamine at 5 mcg/kg/min was infused for 21 minutes. • HR 64 66 • SBP 124 134 • No symptoms • No ECG changes
Clinical Data Should our patient be revascularized?
Dysfunctional but Viable Myocardium LVEF 32% LVEF 54% Horn HR, Teichholz LE, Cohn PF, Herman MV, Gorlin R. Augmentation of left ventricular contraction pattern in coronary artery disease by an inotropic catecholamine: the epinephrine ventriculogram. Circulation 1974;49:1063-1071
Dysfunctional but Viable Myocardium • Hibernating • Chronic ischemia or repetitive stunning • Ultrastructural changes that result in • Disassembly of contractile apparatus • Recovery in weeks or months after revascularization • Stunned • Acute ischemia • No ultrastructural changes • Recovery in minutes to days after revascularization
CABG in Patients with LV Dysfunction Chareonthaitawee et al, JACC 2005;46:567
Importance of Viable Myocardium J Am Coll Cardiol 2002;39:1151
Evaluation of Viability Chareonthaitawee et al, JACC 2005;46:567
Nuclear Techniques • SPECT • 201Tl • 99mTc • 123I Fatty Acids • PET Agents • PET • 18FDG • 11C Acetate
SPECT • 201Tl most commonly used • Several protocols for use • Stress – redistribution • Rest – redistribution • Usually imaged 4 to 24 hours after initial injection • With or without reinjection • Usually at 4 hours • Perfusion tracer initially • Ischemia is a sign of viability • Membrane integrity tracer in the late phase • K analog • Assesses integrity of membrane and Na-K-ATPase
SPECT • 99mTc also helpful • Stress – rest protocol • Perfusion tracer • Ischemia is a sign of viability • Membrane integrity tracer • Trapped by active mitochondria • PET agents act as with PET imaging
201Tl Uptake and Recovery of Function Perrone-Filardi P, Pace L, Pratarto M, et al. Dobutamine echocardiography predicts improvement of hypoperfused dysfunctional myocardium after revascularization in patients with coronary artery disease. Circulation. 1995;91:2556-2565.
Comparison of 201Tl and 99mTc Udelson JE, Coleman PS, Metherall J, et al. Predicting recovery of severe regional ventricular dysfunction. Comparison of resting scintigraphy with 201Tl and 99mTc-sestamibi. Circulation. 1994;89:2552-2561.
PET • All PET agents (18FDG, 11C acetate) assess cardiac energy metabolism. • 18FDG imaging assesses glucose metabolism • Ischemic myocardium generally favors glucose utilization • 11C acetate imaging assesses lipid metabolism
Importance of Good Patient Preparation • In the assessment of myocardial viability, the quality and utility of the images is highly dependent on appropriate patient preparation • Inadequate patient preparation can lead to spurious results or images with no diagnostic value
Myocardial Energy Metabolism • Cardiac myocytes are continuously active • Require efficient use of energy resources • Require continual repletion of energy substrates • Faced with varying levels in supply • Flexibility in substrate use
Anaerobic Metabolism • Inefficient • Each glucose molecule yields two ATP • Requires glucose • Does not require oxygen • Lactate is the waste product Based on Autumn Cuellar (Bioengineering Institute, University of Auckland)
Aerobic Metabolism • Efficient • Citric acid cycle produces abundant ATP • Can function with multiple substrates • Requires oxygen • Water and CO2 are the waste products Based on Autumn Cuellar (Bioengineering Institute, University of Auckland)
Myocardial Energy Metabolism ketone bodies amino acids Based on Autumn Cuellar (Bioengineering Institute, University of Auckland)
Myocardial Energy Metabolism ketone bodies amino acids Based on Autumn Cuellar (Bioengineering Institute, University of Auckland)
Glucose Handling • Largely determined by the availability of glucose in the blood stream • Insulin is the major regulatory hormone
Glucagon Glucose Handling: Fasting
Glucose use Gluconeogenesis Glycogen FFA Glucagon Glucose Handling: Fasting
Glucose use Gluconeogenesis Glycogen Fat storage Glucose Handling: Fed
Glucose Handling: Fed Glucose use Gluconeogenesis Glycogen Fat storage
Glucose use Gluconeogenesis Glycogen FFA Glucose Handling: Diabetes (1)
Glucose use Gluconeogenesis Glycogen FFA Glucose Handling: Diabetes (2)
Glucose Handling • In normal patients, feeding causes a rise in glucose and insulin that restores glucose balance • Uptake of glucose in peripheral tissues • HEART • In type 1 diabetics, feeding causes a rise in glucose while insulin remains low/absent • Continued gluconeogenesis and glucose conservation • In type 2 diabetics, feeding causes a rise in glucose and insulin but peripheral tissues are resistant to the action of insulin • Continued gluconeogenesis and glucose conservation
FDG FDG: C6H11O5 Glucose: C6H12O6