Testicular microlithiasis
Testicular microlithiasis. By Dr. Wissam Kh. Kamal R2 Urology KAUH. ??? Testicular Microlithiasis ??? ??????. Introduction. Incidence. Etiology. Diagnosis. Clinical correlations. Management. Conclusion.

Testicular microlithiasis
E N D
Presentation Transcript
Testicular microlithiasis • By Dr. Wissam Kh. Kamal • R2 Urology KAUH
Introduction. • Incidence. • Etiology. • Diagnosis. • Clinical correlations. • Management. • Conclusion.
Testicular Microlithiasis or polytopic intralobular calcifications is uncommon urologic entity of unclear etiology. • It is usually an incidental finding during investigation of unrelated testicular symptoms by scrotal sonography. • Prior to the clinical application of high resolution U/S, TM was a histological diagnosis established on autopsy or orchiectomy / testicular biopsy specimens. • The term “Testicular Microlithiasis” was used only when a significant number of seminiferous tubules contained microliths.
Infertility. Testicular atrophy. Cryptorchidism or delayed testicular descent . Varicocele. Testicular torsion. Male pseudohermaphroditism. Pulmonary alveolar microlithiasis. Calcification of the sympathetic nervous system. Down’s, Kleinfelter and Carney’s syndroms and cystic fibrosis. It’s occurrence in otherwise normal testes has also been reported. TM has been observed in patients with:
Incidence • The true incidence of TM is unknown due to a limited number of cases, significant differences in studied populations, diagnostic methods and undefined prevalence of TM in normal individuals. • Autopsy revealed TM in 0.04 to 11.8 % of prepubertal boys and 3% of adult males. • Nistal et al reported TM in 1 of 618(0.16%) testicular biopsy specimens performed in children. • In a retrospective analysis of 1710 testicular sonograms of adults, bilateral TM was demonstrated in 11 cases (0.6).
To answer the question of how common testicular microlithiasis is in an asymptomatic population a prospective U/S screening study was made to establish the prevalence of the condition in a healthy population of men undergoing annual training for the U.S army. • A total of 1504 male participants were evaluated using physical examination and testicular U/S.
TM was present in 84 (5.6%) and was bilateral in 66.7 % with the majority having 5-25 microcalcification per testicle on U/S. • The frequency of detection of testicular microlithiasis in relationship to the racial background of the study participants was 4.2% White, 14.1% African-American, 8.5% Hispanic, 5.6% Asian or Pacific Islander and 5.2% who did not claim a race affiliation.
The origin of these intrtubular calcification is unclear. • Numerous theories have been proposed including liquefaction of protoplasmic dendritus about a spermatocyte or coalescence of colloid droplets, ectopic oocytes in dysgenetic testes, displaced spermatogenia, undifferentiated, or desquamated calcified cells, depostion of glycoprotien about a nidus of cell material sloughed into the tubular lumen and abnormal Sertoli cells activity.
After the application of electron microscopy; vacoulized degenerating cells not phagocytized by Sertoli cells were suggested to form the nidus for microlith with the tubular lumen. Further development of microliths may resemble the crystal-matrix formation of urinary calculi. • In two cases TM has been associated with pulmonary microlithiasis and calcifications in the sympathetic nervous system and brain. • This suggests the possibility of alteration in the chemical composition of certain mucosubstances which would enhance the deposition of Calcium in different organs. • A systemic calcium metabolic disorder has been hypothesized but never proven.
Since TM was found in patients with Klinefelter’s, Down’s and Carney’s syndroms and recently with cystic fibrosis, genetic disorders were thought to play a role in the development of TM and chromosomal analysis was suggested for patient evaluation.
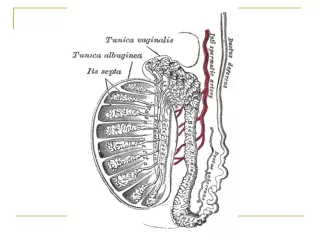
Histology • On histologic examination microliths (also called calcospherites) are eosinophylic, spherical, elongated or ovoid in shape. • Under the light and electron microscope the microliths are found to consist of two zones: a central calcified zone and a multilayered envelope of stratified collagen fibers.
The histological appearance of the remaining epithelium varies according to the patient’s age and associated conditions ( e.g. cryptorchidism, infertility, CIS). • The uninvolved tubule segments were lined largely by undifferentiated cells with increased cytoplasmic swelling. • Spermatogonia were clearly identified within the tubules in normal numbers, but most tubules had a narrow or no lumen.
Ultrasound • The ultrasound appearance of TM was first described by Doherty et al. in 1987 as; innumerable tiny bright echoes diffusely and uniformly scattered throughout their substance. • This sonographic appearance was further defined by Doherty and Janzen as ` randomly distributed 1-2 mm diameter hyperechoic foci in one or both testes.
The classical description of TM is bilateral evenly distributed bright echoes. • TM has been divided into classic TM (with five or more microliths on any single view) and limited TM (less than 5 microliths). • It has been graded as minimal/mild (grade1), moderate(grade2), and severe(grade3). • This variable pattern was directly correlated with the frequency of occurrence of testicular malignancy.
Large, less numerous, less well defined and commonly unilateral hyperechoic areas on testicular U/S were described in patients with orchitis, sarccoidosis, local infarction, calcified granulomas and focal scars, large-cell calcifying Sertoli cell tumors, tubular atrophy with fibrosis or calcifications in germ-cell tumors and adrenal rests. • The lack of uniformity and the liberal definition of TM in the literature make it more difficult to correlate the spectrum of U/S findings with clinical diagnosis in different studies.
Clinical Picture • TM is usually asymptomatic but occasionally may be associated with orchialgia. • Ducheket al presented one case of painful testicular microlithiasis in an otherwise healthy 22-year old patient. • The mechanism of pain was suggested to be a distention of seminiferous tubules. • Mackinnon reported five patients with orchialgia and infertility with TM diagnosed in four of them.
Infertility • The relationship between TM and fertility is not well understood. • In Janzen’s series of 11 patients with TM, two(18 %) presented with infertility. • Hobarth et al and Mackinnon et al reported oligo- or azospermia in 19 and 80 % of their patients with TM respectively.
It was suggested that microliths and infertility may have a common undefined etiologic factor. • Fertility potential may be decreased by a mechanical obstruction of seminiferous tubules with microliths, atrophy of uninvolved tubules with spermatogenic arrest or a combination of both. • Limited cases of testicular biopsy in patients with infertility and TM revealed microliths in 30 to 40% of the seminiferous tubules with obstruction.
Mackinnon et al suggested testicular U/S in the work up of male infertility, although it’s not usually recommended. • The prognosis of fertility is not necessarily affected by microlithiasis. • In a case of bilateral TM, bilateral varicocele and normal spermatogenesis, pregnancy was achieved after bilateral varicocelectomy. • Incidentally, discovered TM should not change the treatment approach to infertile men.
Malignancy • The evaluation of testicular biopsy or orchiectomy specimens and total specimen radiography identified the coexistence of intratesticular microcalcification and malignancy. • Wurster and Menges retrospectively found microcalcifications in 46% of 127 germ cell tumors. • Only 8 of 49 (16%) specimens of benign testicular disorders( cryptorchidism, epididymitis, torsion) revealed microcalcifications.
TM is most commonly associated with non-seminoma germ cell tumor. • The association between TM and Testicular CIS has been well documented. • In a retrospective study of testicular specimens with CIS, but without testicular tumor; Kang et al found TM in 14 of 36(39%) specimen compared to 2.1% in controlled group. • The limited results of prospective follow up studies of asymptomatic patients with TM are controversial.
Janzen found no interval malignancy in six patients with classical bilateral TM within 14-49 months. • Hobarth observed 16 patients with bilateral TM and unilateral testicular tumor. No contralateral tumors developed from 6-65 months. • Whitman followed 21 patients with TM clinically and sonographically between one and nine years and no patients developed interval malignancy.
Although most tumors were detected simultaneously with TM recently cases in testicular malignancy developing after diagnosis of testicular microlithiasis have been reported.
McEniff et al presented a case of yolk sac tumor of the testis developing in a 17 Y/O boy with TM 4 years after initial evaluation of a unilaterally enlarged testis. • Winter et al reported a case of unilateral microlithiasis in a 21 Y/O man with bilateral testicular pain and hematospermia. Three years later an U/S revealed a multifocal solid testicular mass (embryonal cell carcinoma and seminoma) in the involved testis.
Frush et al described a patient with unilateral microliths and subsequent (15 month later) development of mixed germ cell tumor in the involved testis. Interestingly microliths were diagnosed also in the uninvolved testis. • Kaveggia et al presented a case of unilateral testicular seminoma with contralateral TM. Three years later after radical orchiectomy and radiation treatment ( contralateral testis was not shielded) the patient was diagnosed with CIS in the remaining testis and underwent orchiectomy.
TM is often found in patients with cryptorchidism, testicular atrophy and infertility. These conditions have been associated with an increased risk of developing CIS and testicular tumor. • It has been proposed that TM is a manifestation of primary testicular dysfunction and this dysfunction is associated with a higher prevalence of testicular malignancy.
The development of Tumors in some testes with microliths were shown years after presentation, therefore TM is thought to be a predisposing factor, a possible indirect indicator of premalignant disease or a tumor marker.
There is a significant risk of testicular neoplasms in patients with TM. • Since most patients with either TM or germ cell tumor are 20 to 50 years old, prompt evaluation of TM in this age group is indicated. • Serial physical examination, serum tumor markers and high resolution testicular U/S are recommended to rule out associated malignancy.
If no testicular malignancy is present, 6-12 month intervals of clinical, U/S surveillance and annual tumor markers are suggested. • If future studies confirmed a strong association between TM and CIS, TM maybe viewed a specific marker of testicular malignancy and an indication of testicular biopsy. • Presently the results of limited studies and case reports do not justify routine testicular biopsy in patients with typical U/S appearance of TM.
Indications for Testicular Biopsy: • Focal clumped and unilateral TM without mass. • TM in infertile men, patients with cryptorchidism and/ or atrophic testes. • Patients with ipsilateral testicular tumor and TM in the contralateral testis.
Although TM by itself is a benign disease which does not require treatment, the association of TM with testicular malignancy is clinically important. • Careful evaluation and follow up of asymptomatic patients with incidentally diagnosed TM is recommended. • It is especially indicated for the patients with cryptorchidism, infertility, testicular atrophy and contralateral testicular tumor who are at high risk for harboring and developing malignancy.
The patient should be educated about the known association between TM, testicular tumor and CIS and instructed in testicular self examination as well as the need for semi-annual / annual testicular U/S, physical exam and tumor marker. • It is reasonable to consider biopsy in high risk patients only if treatment of CIS is planned.
References • AUA series. • Current opinion in Urology 2007. • Cambpel the 9th edition.
Thank You Dr. Wissam Kh. Kamal R2 Urology