Chapter 19- Blood
Chapter 19- Blood. Functions of Blood. Substance distribution : Oxygen from the lungs and nutrients from the digestive tract Metabolic wastes from cells to the lungs and kidneys for elimination Hormones from endocrine glands to target organs Regulation :

Chapter 19- Blood
E N D
Presentation Transcript
Functions of Blood Substance distribution: Oxygen from the lungs and nutrients from the digestive tract Metabolic wastes from cells to the lungs and kidneys for elimination Hormones from endocrine glands to target organs Regulation: Appropriate body temperature by absorbing and distributing heat Normal pH in body tissues using buffer systems Adequate fluid volume in the circulatory system
Functions of Blood Body protection prevents blood loss by: Activating plasma proteins and platelets Initiating clot formation when a vessel is broken Blood prevents infection by: Synthesizing and utilizing antibodies Activating complement proteins Activating WBCs to defend the body against foreign invaders
Physical Characteristics and Volume Color varies from scarlet to dark red The pH of blood is 7.35–7.45 Temperature is 38C Blood accounts for approximately 8% of body weight Average volume: 5–6 L for males, and 4–5 L for females
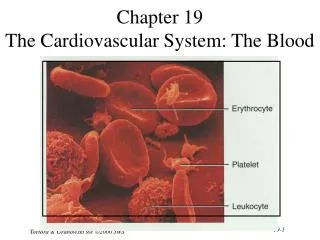
Composition of Blood What type of tissue is blood? It is composed of liquid plasma (matrix) and formed elements Formed elements include: Erythrocytes, or red blood cells (RBCs) Leukocytes, or white blood cells (WBCs) Platelets
Blood Plasma Blood plasma contains over 100 solutes, including: Proteins – albumin, globulins, clotting proteins, and others Lactic acid, urea, creatinine Organic nutrients – glucose, carbohydrates, amino acids Electrolytes – sodium, potassium, calcium, chloride, bicarbonate Respiratory gases – oxygen and carbon dioxide
Accounts for 46-63% of blood volume 92% of plasma is water In many respects, plasma composition resembles that of the interstitial fluid The differences between plasma and interstitial fluids are: Concentration of dissolved oxygen and carbon dioxide Concentration of dissolved proteins (plasma proteins can not cross capillary walls) Plasma
Blood Plasma proteins • 8% of plasma weight • Contribute to osmotic pressure • Proteins are mostly produced by the liver • 60% albumin • 36% globulins • 4% fibrinogen
Formed Elements Erythrocytes, leukocytes, and platelets make up the formed elements Only WBCs are complete cells RBCs have no nuclei or organelles, and platelets are just cell fragments Most formed elements survive in the bloodstream for only a few days Most blood cells do not divide but are renewed by cells in bone marrow
What is the function of erythrocytes? • What elements in their structure support their function? • Function – carry respiratory gases – mainly oxygen • They contain hemoglobin and have a biconcave structure that helps with moving into small blood vessels
Erythrocytes (RBCs) Biconcave discs, anucleate, essentially no organelles Filled with hemoglobin (Hb), a protein that functions in gas transport The biconcave disc shape provides a large surface to volume ratio – help with fast exchange between the cell and the plasma allows RBCs to stack – facilitate flow through narrow blood vessels Allows the RBCs to bend and flex when entering small capillaries Structural characteristics contribute to its gas transport function Erythrocytes are more than 97% hemoglobin ATP is generated anaerobically through glycolysis (they lack mitochondria), so the erythrocytes do not consume the oxygenthey transport
The hematocrit (also called volume of packed red cells, VPRC, or packed cell volume, PCV) is a measure of the relative percentage of blood cells (mainly erythrocytes) in a given volume of whole blood. Normal hematocrit for Adult Females: 37-48% (ave. 42%) Normal hematocrit for Adult Males: 42-52% (ave. 47%) Hematocrit Measurement
RBC membranes have glycoprotein antigens on their external surfaces These antigens are: Unique to the individual Recognized as foreign if transfused into another individual Promoters of agglutination and are referred to as agglutinogens Presence or absence of these antigens is used to classify blood groups Human Blood Groups
The ABO blood groups consists of: Two antigens (A and B) on the surface of the RBCs Two antibodies in the plasma (anti-A and anti-B) ABO blood groups may have various types of antigens and preformed antibodies Agglutinogens and their corresponding antibodies cannot be mixed without serious hemolytic reactions ABO Blood Groups
Blood Typing When serum containing anti-A or anti-B agglutinins is added to blood, agglutination will occur between the agglutinin and the corresponding agglutinogens Positive reactions indicate agglutination
Transfusion reactions occur when mismatched blood is infused Donor’s cells are attacked by the recipient’s plasma agglutinins causing: Diminished oxygen-carrying capacity Clumped cells that impede blood flow Ruptured RBCs that release free hemoglobin into the bloodstream Circulating hemoglobin precipitates in the kidneys and causes renal failure Transfusion Reactions
There are eight different Rh agglutinogens, three of which (C, D, and E) are common Presence of the Rh agglutinogens on RBCs is indicated as Rh+ Anti-Rh antibodies are not spontaneously formed in Rh– individuals However, if an Rh– individual receives Rh+ blood, anti-Rh antibodies form A second exposure to Rh+ blood will result in a typical transfusion reaction Rh Blood Groups
RH factor blood grouping system • A person with Rh- blood can develop Rh antibodies in the blood plasma if he or she receives blood from a person with Rh+ blood, whose Rh antigens can trigger the production of Rh antibodies. • A person with Rh+ blood can receive blood from a person with Rh- blood without any problems.
Homeostatic Imbalance: Hemolytic Disease of the Newborn • Also called erythroblastosis fetalis • Rh– mother becomes sensitized when exposure to Rh+ blood causes her body to synthesize anti-Rh antibodies • Anti-Rh antibodies cross the placenta and destroy the RBCs of an Rh+ baby • The baby can be treated with prebirth transfusions and exchange transfusions after birth • RhoGAM serum containing anti-Rh can prevent the Rh– mother from becoming sensitized
Erythropoiesis requires: Proteins, lipids, and carbohydrates Iron vitamin B12, and folic acid (necessary for DNA production) Location of iron in the body The body stores iron in Hb (65%), the liver, spleen, and bone marrow Intracellular iron is stored in protein-iron complexes such as ferritin and hemosiderin Circulating iron is loosely bound to the transport protein transferrin Dietary Requirements of Erythropoiesis
RBC formation and turnover The life span of an erythrocyte is 100–120 days Old RBCs become rigid and fragile, and their Hb begins to degenerate RBC travels about 700 miles in 120 days and is being colliding in other RBCs or the vessels walls The damage in the RBC is detected by phagocytes that engulf the RBCs RBCs are replaced at a rate of approximately 3 million new blood cells entering the circulation per second.
Anemia – blood has abnormally low oxygen-carrying capacity It is a symptom rather than a disease itself Blood oxygen levels cannot support normal metabolism Signs/symptoms include fatigue, paleness, shortness of breath, and chills Hemorrhagic anemia – result of acute or chronic loss of blood Hemolytic anemia – prematurely ruptured RBCs Aplastic anemia – destruction or inhibition of red bone marrow Erythrocyte Disorders
Iron-deficiency anemia results from: A secondary result of hemorrhagic anemia Inadequate intake of iron-containing foods Impaired iron absorption Pernicious anemia results from: Deficiency of vitamin B12 Lack of intrinsic factor needed for absorption of B12 Treatment is intramuscular injection of B12 Anemia: Decreased Hemoglobin Content
Anemia: Abnormal Hemoglobin Sickle-cell anemia – results from a defective gene coding for an abnormal Hb called hemoglobin S (HbS) HbS has a single amino acid substitution in the beta chain This defect causes RBCs to become sickle-shaped in low oxygen situations
Anemia: Abnormal Hemoglobin • Thalassemias – absent or faulty globin chain in Hb • RBCs are thin, delicate, and deficient in Hb http://pathy.med.nagoya-u.ac.jp/atlas/img/t2/img0027.jpg
Erythrocyte Disorders - polycythemia • Polycythemia: excess of RBCs that increase blood viscosity • Results from: • Polycythemia vera — bone marrow cancer • Secondary polycythemia — when less O2 is available (high altitude) or when EPO production increases • Blood doping – increase RBC by infusion or by injections of erythropoietin
Leukocytes (WBCs) • Leukocytes, the only blood components that are complete cells: • Are less numerous than RBCs • Make up 1% of the total blood volume • Can leave capillaries via diapedesis • Move through tissue spaces • Leukocytosis – WBC count over 11,000 / mm3 • Normal response to bacterial or viral invasion
Types of WBC • Five types of WBC: neutrophils, eosinophils, basophils, monocytes, lymphocytes • First 4 are part of the body non-specific defense and lymphocytes are part of the specific defense (will be discussed later in the course) • WBC are divided into 2 groups on the basis of their appearance after staining: • Granulocytes – visible stained granules • Agranulocytes – non-visible granules
Granulocytes • Granulocytes – • Neutrophils – netural granules • Eosinophils – acidic staining • Basophils – basic staining • Contain cytoplasmic granules that stain specifically (acidic, basic, or both) with Wright’s stain • Are larger and usually shorter-lived than RBCs • Have lobed nuclei • Are all phagocytic cells
Neutrophils • 50-70% of WBC • Segmented nuclei with 2-5 lobes (polymorphonuclear) • Highly mobile • First to arrive to site of injury • Attack and digest bacteria that have been marked with antibodies (Ab) • Contain peroxidases, hydrolytic enzymes, and defensins (antibiotic-like proteins) • Short life span (~10d); if activated live 30min or less • Breakdown of a neutrophil releases chemicals that attract other neutrophils
Eosinophils • Eosinophils account for 1–4% of WBCs • Have bilobed nuclei connected via a broad band of nuclear material • Have red to crimson (acidophilic) large, granules • attack parasites and phagocyte antigen-antibody complexes
Basophils • Account for 0.5% of WBCs • Have U- or S-shaped nuclei • The staining of the granules is dark and obscure the nucleus • Have large, purplish-black (basophilic) granules that contain histamine • Histamine – inflammatory chemical that acts as a vasodilator and attracts other WBCs (antihistamines counter this effect) • In the site of injury releases granules that contain histamine (vassodilator) and heparin( prevents clotting)
Agranulocytes • Agranulocytes: lymphocytes and monocytes • Lack visible cytoplasmic granules • Have spherical or kidney-shaped nuclei
Lymphocytes • Account for 25% or more of WBCs • Have large, dark-purple, circular nuclei with a thin rim of blue cytoplasm • Are found mostly in lymphoid tissue (some circulate in the blood) • There are two types of lymphocytes: • T cells function in the immune response • B cells give rise to plasma cells, which produce antibodies
Monocytes • Monocytes account for 4–8% of leukocytes • They are the largest leukocytes • They have abundant pale-blue cytoplasm • They have purple-staining, U- or kidney-shaped nuclei • They leave the circulation, enter tissue, and differentiate into macrophages
Leukopoiesis • Production of WBCs • Stimulated by chemical messengers from bone marrow and mature WBCs • Interleukins (e.g., IL-1, IL-2) • Colony-stimulating factors (CSFs) named for the WBC type they stimulate (e.g., granulocyte-CSF stimulates granulocytes) • All leukocytes originate from hemocytoblasts
Leukocyte Disorders • Leukopenia • Abnormally low WBC count—drug induced • Leukemias • Cancerous conditions involving WBCs • Named according to the abnormal WBC clone involved • Myelocytic leukemia involves myeloblasts • Lymphocytic leukemia involves lymphocytes
Leukemia • Bone marrow totally occupied with cancerous leukocytes • Immature nonfunctional WBCs in the bloodstream • Death caused by internal hemorrhage and overwhelming infections • Treatments include irradiation, antileukemic drugs, and stem cell transplants
Platelets • Small fragments of megakaryocytes • Formation is regulated by thrombopoietin • Blue-staining outer region, purple granules • Granules contain serotonin, Ca2+, enzymes, ADP, and platelet-derived growth factor (PDGF)