Hypothesis
Hypothesis. Our next hypothesis: After a 2 year hiatus, does resuscitation skill performance and HFHS trained individuals improve to a greater percentage than traditionally trained didactic only individuals following a didactic only refresher if the team is physician led?. Methods. n= 234

Hypothesis
E N D
Presentation Transcript
Hypothesis Our next hypothesis: After a 2 year hiatus, does resuscitation skill performance and HFHS trained individuals improve to a greater percentage than traditionally trained didactic only individuals following a didactic only refresher if the team is physician led?
Methods n= 234 Twenty-six teams of 9 Subjects were selected from students coming in randomly for ACLS Refresher training. Teams were formed based on their exposure to HFHS or not.
Methods Previous returning students who had obviously been exposed to HFHS were assigned to the HFHS teams. Subjects who were assigned to the traditional group were based on a review of our records which showed they had not attended any of our courses, not even Health Care Provider CPR with our simulators.
Methods Our database (Training Manager) randomizes the names. We have no control of how the students name appear on the roster or in the order in which they appear. It does not alphabetize. When a course roster is printed, team leaders were selected from the top of the list.
Methods The next step was to find a Respiratory Therapist or Anesthesiologist to fill the Advanced Airway position, and lastly, all nurses filled team member positions, from the top of the list, down. The investigators were blinded, having no knowledge of which team was being observed.
Methods • As the subjects arrived they received their team badge and written code room instructions and student survey. • Once they were all seated, our administrative assistant would select which team came into the learning lab first.
Methods • Once assembled, the team received oral instructions which were read from a prepared paper about what the HFHS could do as well as the defibrillator and medications available in the crash cart. Recording sheets and AHA crash cart cards were available for each simulation.
Methods • Each simulation scenario lasted ten minutes. • Each team received the same scenario of a patient in V-fib cardiac arrest.
Methods 3 measurements were taken: First V-fib resuscitation of the simulator before any training was received. Second, following a 4 hour lecture covering the AHA Guidelines and practicing High-quality CPR and using an AED
Methods Finally, Last V-fib resuscitation of the training day.
Methods Team leadership and individual skills were evaluated using video tape and SimMan event logs printed for each of the resuscitations. Time to task completion was marked for each task using the AHA Guideline Model.
Methods • Start CPR • Defib #1 • CPR • Defib #2 • CPR • Epinephrine #1 • Defib #3 • CPR • Amiodarone • Epinephrine #2 • Defib #4 • CPR We constructed an AHA Guidelines model which looked at specific tasks and time to completion.
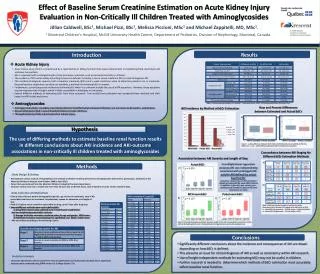
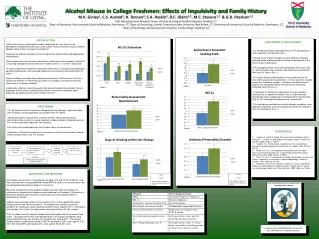
Results Poster Presentation RESS 2010 • The level of compliance of treating a HFHS in V-fib in compliance with the AHA Guidelines following a 2 year hiatus before any training was the same for both groups, less than 30%.
Results Following a 4 hour lecture covering the AHA Guidelines and practicing High-quality CPR and using an AED. The level of compliance of treating a HFHS in V-fib increased to 55% as compared to the traditional trained group which was at 40%.
Results Following a 4 hour lecture covering the AHA Guidelines and practicing High-quality CPR and using an AED, and practice codes. The level of compliance of treating a HFHS in V-fib increased to 75% as compared to the traditional trained group which was at 60%.
Conclusion • Following a 2 year hiatus in ACLS training, there appears to be a significant degradation of skills and knowledge to a level that may be insufficient for effective resuscitation, regardless of the training modality.