Hypothesis
Explore evidence, sources, and reduction of oxidative stress in preeclampsia, proposing antioxidants as prevention via randomized trials. Discuss generation, interactions, and implications of pro-oxidants secondary to abnormal placental perfusion. Investigate placental's role as a source of oxidative stress due to physiological changes like reduced uterine blood flow. Present findings from a clinical trial on antioxidant therapy for preventing endothelial activation in preeclampsia. Discuss implications for future approaches and preventative strategies. Highlight the importance of understanding disease pathogenesis in designing effective prevention trials.

Hypothesis
E N D
Presentation Transcript
Hypothesis • The generation of pro-oxidants secondary to abnormal placental perfusion interacts with maternal constitutional factors to generate oxidative stress.
Questions • Is there evidence of oxidative stress? • What is the source of oxidative stress? • Are antioxidants reduced?
Evidence of oxidative stress in preeclampsia • Increased circulating markers • Lipids (MDA, isoprostanes) • Activated blood cells • Antibodies to ox-LDL • Tissue changes • Increased nitrotyrosine (NO + O) in placenta and maternal vessels • Ascorbate consumption
Questions • Is there evidence of oxidative stress? • What is the source of oxidative stress? • Are antioxidants reduced?
The placenta as a source of oxidative stress Speculation: Uterine blood flow is reduced with uterine contractions. In addition uterine blood flow is not privileged and is decreased with posture and activity. With abnormal implantation might these physiological changes result in a hypoxia reperfusion scenario?
Questions • Is there evidence of oxidative stress? • What is the source of oxidative stress? • Are antioxidants reduced?
XOD Cytokeratin Normal 7 wks Normal 18 wks Normal 34 wks Preeclampsia 28 wks
The definitive question • Can preventing oxidative stress prevent endothelial activation and Stage 2 of preeclampsia?
A (small) randomized controlled trial of antioxidant therapy to prevent preeclampsia Chappell LC, Seed PT, Briley AL, Kelly FJ, Lee R, Hunt BJ, Parmar K, Bewley SJ, Shennan AH, Steer PJ, Poston L. Lancet 1999;354:810-816 • High risk women identified by: • doppler of uterine artery (20 and 24 weeks gestation) • preeclampsia in previous pregnancy • chronic hypertension • previous early onset preeclampsia
Design • positive screened women randomized at 20 weeks to 1 gm ascorbic acid and 400 IU vitamin E (n = 141) or placebo (n = 142) • If doppler not positive at 24 weeks Rx stopped • intent to treat analysis • primary outcome 30% reduction in evidence of endothelial activation (PAI-1/PAI-2)
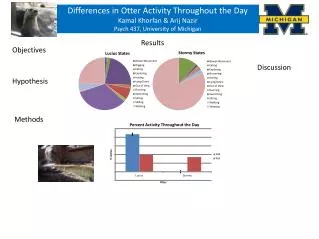
Results • PAI-1/PAI-2 20% with Rx (p < 0.015) • Preeclampsia (p = 0.02) • Placebo 24/142 • Rx 11/141
Stage 1: Reduced Placental perfusion abnormal implantation Stage 2: Maternal Syndrome Oxidative Stress Maternal Constitution: Genetic, Behavioral, Environment Pregnancy Changes
Future approaches • Identify women with predispositions and treat appropriately (e.g.thrombophillia, dyslipidemia) • Antioxidants?
Antioxidants for preeclampsia • Will they work? • Are they safe?
Antioxidant Trial(in preparation) • NICHD/NHLBI/?Canada/?WHO
Design • RCT of vitamin C (1000 mg.) and Vitamin E (400 iU) vs. placebo • Prospective collection of data and biological materials • Primary outcome • severe growth restriction < 3d centile • Infant death after 20 weeks gestation • Power analysis • p < 0.05 and power = 0.8 to detect 30% reduction in primary outcome
Design • Subjects • Nulliparous low risk women (9000) • ? High risk women (3600) • ? Women from low C and E intake areas (WHO)
NICHD Antioxidant TrialsDoes it satisfy the “requirements“? • Should have as primary outcome an endpoint relevant to neonatal well-being. • IUGR and death • Must be large enough to detect adverse fetal/neonatal outcome. • At least 4500 women in each arm
NICHD Antioxidant TrialsDoes it satisfy the “requirements“? • Should have as primary outcome an endpoint relevant to neonatal well-being. • IUGR and death • Must be large enough to detect adverse fetal/neonatal outcome. • At least 4500 women in each arm • Admits our knowledge is limited and collects mechanistic data
Preventing Preeclampsiathe “bottom line“ • Any future clinical trial must be guided by well established pathophysiological information • We must understand a disease before we can prevent it!
Summary • Calcium and aspirin in large clinical trials did not reduce the frequency of preeclampsia • “Hints” from the aspirin trials indicate that the strategy of early treatment may be effective • Increasing data supports diverse maternal factors contributing to the pathogenesis of preeclampsia • Oxidative stress may be the convergence point • Keep your fingers crossed!
Aspirin for PreeclampsiaPrevention trials After Carits et al NEJM 338:701; 1998
Aspirin for PreeclampsiaPrevention trials After Carits et al NEJM 338:701; 1998
Why the Discrepancies?ASA Trial Specific The impact of compliance
Why the Discrepancies?ASA Trial Specific • Wrong dose of ASA? • Wrong timing? • (*time of day and time of pregnancy) • Poor compliance?
Summary • Trials of preeclampsia prevention (early treatment) have not demonstrated clinically relevant effects. • In single center trial with compliance monitoring ASA was minimally effective. • Future studies should identify a relevant target before more trials. • There may be different targets in different subsets of preeclamptic women.
Chlamydia pneumoniaeassociation with vascular disease • Seropositivity is more common • Coronary artery disease • Cerebrovascular disease • Hypertension • Organisms • Present in diseased coronaries • Present in atherosclerotic tissue • Tropism for vascular tissue (smooth muscle and endothelium)
Oxidative stress in preeclampsialinkage of placenta and systemic • Stable products of lipid peroxidation • Activated neutrophils/monocytes • Microvillus fragments