Download
1 / 12
120 likes | 149 Vues
Explore studies on functional recovery after stroke, including motor analysis, management of shoulder pain, and research findings on limb reorganization.

E N D
Recovery of the upper limb function after stroke Wael Alasaq PT. Ph.D. Kuwait University PT Dep.
Functional recovery Reports: • Functional recovery of UL of pt vary from 5%-52% (irrespective of initial impairment severity) Gowland, 1982 & Dean & Mackey, 1992 • 20% of pts with flaccid UL 2 WKs after stroke regained any functional use of the hand. Wade et al 1983 • Absence of a measurable grip by 1 moth after stroke indicate poor functional recovery Sunderland et al 1989
Reports Cont. • +ve effects of interventions involving repetitive exercise & practice of task-oriented & functionally relevant actions. (Sunderland et al 1992, Butefesch et al . 1995, Duncan 1997, Kwakkel et al 1999, Perry et al 1999b, Nelles et al 2001) • +ve effects of intensive task-oriented exercise of the affected limb during constraint of non affected limb in those with some ability to activate hand muscles (Taub et al. 1993, Liepert et al. 2001)
Reports Cont. • Although most recovery occurs within the first 3 mths, training studies have shown improvement in functional UL performance more than 1 year following strike. • This suggests that functional recovery may go on for much longer for those maintaining active use of the limb. • This reflects the nature of brain reorganization as a result of use & activity.
Analysis of motor performance UL functional performance is affected by: • Depressed motor output • Decreased rate of neural activation • Poor timing & coordination of segmental movements • Sensory deficits
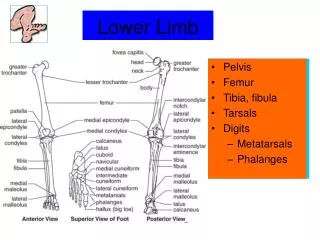
Motor analysis Cont Research findings: • No evidence of proximal to distal recovery. • Weakness of GHJ abductors, flexors & external rotators & of supinators affect reaching actions. • Weakness of wrist extensors, finger & thumb flexors & extensors, abductors & adductors affect manipulation of objects.
Research findings cont. • Reaching movement generally slower after stroke. • Pts perform better in concrete tasks involving meaningful interaction with an object, compared to an abstract task with no object. (Van der Weel et al. 1991) • Reflex hyperactivity, associated reactions & co-contraction do not necessarily interfere with function (O’Dwyer ey al. 1996, Ada & O’Dwyer 2001)
Research findings cont. • Reflex hyperactivity & muscle stiffness respond +vely with vigorous task-specific exercise & training. (Miller & Light 1997, Teixeira-Salmela et al. 1999)
Shoulder Pain • 84% of pt develop shoulder pain following stroke. (Najenson et al. 1971, van Ouwenaller et al. 1986, Roy et al. 1994) • With some pts pain start to develop as early as 2 Wks after stroke (Brocklehurst et al. 1978) • Decreased in the pain-free range of movement occur within the first 2 WKs. (Buhannon & Andrews 1990) • Subluxation may occur within 3 WKs (Chaco & Wolf 1971)
Shoulder Pain Cont. • Shoulder pain interferes with rehabilitation & has –ve effect on functional recovery. • Factors causing shoulder pain • Pre-stroke factors (degeneration) • Post-stroke factors (immobility, soft tissue changes, disuse, trauma etc) • Pain is mostly due to • Development of adhesive capsulitis • Pinching of stretched soft tissue between joint surfaces.
Management of shoulder pain • Injection of anti-inflamatory or analgesic substances • TENS • Passive joint mobilization • Active exercises
Prevention Prevention Prevention • Positioning • Pain-free active exercise • Electrical stimulation: Anterior & posterior deltoid muscle. • Avoid damaging activities, such as pulling, passive ROM exercises