Download
1 / 73
750 likes | 1.15k Vues
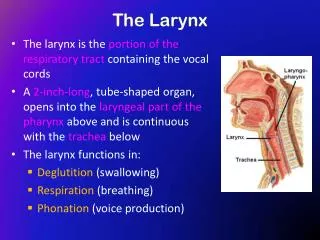
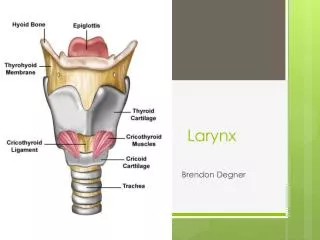
Case Studies in the Larynx Non-SCC Pathology. Nicholas S. Pierson, MD University of Utah Neuroradiology 12 th Intensive Interactive Head and Neck Imaging Conference. Objectives. Case based review of key laryngeal diagnoses and imaging characteristics

E N D
Case Studies in the LarynxNon-SCC Pathology Nicholas S. Pierson, MD University of Utah Neuroradiology 12th Intensive Interactive Head and Neck Imaging Conference
Objectives • Case based review of key laryngeal diagnoses and imaging characteristics • Dispel the myth that “the only thing that happens in the larynx is SCC” • Provide appropriate differential diagnoses • Introduce some uncommon pathologies of the larynx
Case 1 • 49 year old male • Progressive difficulty breathing • Globus sensation • 30 pack year smoking history
DDX • Polyp • Nodule • Polypoid degeneration • Squamous papilloma • SCC
Vocal Cord Polyp • Small exophytic growth from the true cord • Usually solitary • Present with hoarseness, breathiness, vocal fatigue, decreased vocal range • Proposed causes: vocal abuse, GERD, nasosinusitis, irritants
Companion Case 1a Vocal Cord Nodule
Case 2 • 75 year old male with hoarseness • Obvious mass on laryngoscopy • Abnormality found incidentally on imaging 10 years prior • Refused treatment at the time
T1 T1 FS Post T2 FS
DDX • Chondroid lesion: Chondroma\sarcoma • Other sarcomas • Inflammatory cartilaginous processes such as relapsing polychondritis • SSC • Rare lesions: Carcinoid, paraganglioma, giant cell tumors • Mets/Myeloma
Low Grade Chondrosarcoma • Expansile mass within laryngeal cartilage • Cricoid most common • Can contain calcified matrix, ring-like or popcorn • Difficult to exclude SCC in non-calcified lesions • Present with dysphagia, dysphonia, or stridor
Companion Case 2a: • 67 year old male • Incidental lesion seen on MRI C-spine • Asymptomatic
39 year old male Difficulty breathing Companion Case 2b:
Case 3: • 64 year old male • History of multiple myeloma and right inguinal melanoma • Metastatic workup
T2 FS T1 T1 FS Post Multiple Myeloma
Companion Case 3a: • 76 year old male • History of multiple myeloma
Companion Case 3b: • 71 year old male • History of prostate cancer
Companion Case 3c: Pitfall • 74 year old male with skull base lesion • Surgical debulking of the left skull base and orbit many years prior • Dysphonia, dysphagia
Vocal Cord Medialization Pitfall • Some patients who have primary malignancies develop vocal cord paralysis • Some of these patients undergo vocal cord medialization • These have variable appearances and can look mass like • Can also be hot on PET
Case 4 • 55 year old male with dysphagia • Fluctuant neck mass • Changes in size and tenderness • Occasional copious secretions
T2 FS
DDX • Laryngocele • Other cystic neck masses • Thyroglossal duct cyst • Branchial cleft cyst 2 and 4 • Lateral hypopharyngeal pouch • Abscess • Vallecular cyst • Cystic nodal mass
External (mixed) Laryngocel • Paraglottic/Supraglottic • Extend through the thyrohyoid membrane • Circumscribed, thin walled, may contain fluid or air • Present as neck mass in low submandibular space
Laryngocele Types • Internal/Simple: confined to paraglottic space • External/Mixed: internal and external components • Pyolaryngocele: superinfection • Secondary: Glottic or inferior supraglottic mass obstructs laryngeal ventricle
Companion Case 4b • 88 year old female with papillary thyroid cancer and lung cancer • 70 year history of ~5 cigarettes per day • Hoarseness • CT STN as part of workup
34 year old mixed martial artist 2 days following tournament Throat injury with progressive pain and difficulty breathing Case 5
8/2013 8/2012
Thyroid Cartilage Fracture • Can be caused by any trauma involving neck: blunt, hanging, penetrating • Include cartilages in search pattern • Important to exclude to avoid airway compromise • When present evaluate surrounding soft tissue and airway • May be a subtle finding
Companion Case 5a • Equestrian injury
Case 6 • 38 year old female • 8 weeks of hoarseness
T1 T2 T1 Post T1 Post
Vocal Cord Paralysis • Sail sign- ballooned ventricle • Medial rotation of arytenoid • Medializedaryepiglottic fold • Enlarged pyriform sinus
Vocal Cord Paralysis • Extensive DDX: Injury to CN10 or RLN anywhere from medulla to AP window • Trauma, neoplasm, idiopathic, stroke • Checklist: Medulla, Jugular foramen, carotid space, TE grove, mediastinum
Companion Case 6a • 73 year old male • Extensive smoking history • Hoarseness
Companion Case 6b • 43 year old male • Acute Horner’s syndrome and nystagmus