Chapter 5: The Skeletal System
Chapter 5: The Skeletal System. Anatomy & Physiology Ms. Halbohm. The Skeleton:. The Skeleton is divided into two subdivisions: 1) The axial skeleton , the bones that form the longitudinal axis of the body 2) The appendicular skeleton, the bones of the limbs and girdles

Chapter 5: The Skeletal System
E N D
Presentation Transcript
Chapter 5: The Skeletal System Anatomy & Physiology Ms. Halbohm
The Skeleton: • The Skeleton is divided into two subdivisions: • 1) The axial skeleton, the bones that form the longitudinal axis of the body • 2) The appendicular skeleton, the bones of the limbs and girdles • In addition to bones, the skeletal system includes joints, cartilages, and ligaments.( fibrous cords that bind the bones together at joints.)
Functions of Bones: • 1) Support: bones form the internal framework that supports and anchors all soft organs. • 2) Protection: Bones protect soft body organs. The skull for example protects your brain. • 3) Movement: Skeletal muscles are attached to bones by tendons and use the bones as levers to move the body and its parts. • 4) Storage: Fat is stored in the internal cavities of bones. Bones also store minerals, the most important being calcium and phosphorus, although others are also stored. • 5) Blood cell formation: Blood cell formation, or hematopoiesis, occurs within the narrow cavities of certain bones.
Classification of Bones: • There are 206 bones in the adult skeleton and two basic types of osseous, or bone tissue: • 1) Compact bone is dense and looks smooth and homogenous. • 2) Spongy bone is composed of small needlelike pieces of bone and lots of open space.
Classification of bones: • 3. Long bones: are typically longer than they are wide. Long bones are mostly compact bones. All the bones of the limbs, except the wrist and ankle bones, are long bones. • 4. Short bones: are generally cube-shaped and contain mostly spongy bone. The bones of the wrist and ankle are short bones. • 5. Flat bones: are thin, flattened, and usually curved. They have two layers of compact bone sandwiching a layer of spongy bone between them. Most bones of the skull, the ribs, and the sternum (breastbone) are flat bones. • 6. Irregular bones are bones that do not fit into any other category. The vertebrae and the hip bones are examples of irregular bones.
Structure of the long bone: • 1. The Diaphysis, or shaft, makes up most of the bone’s length and is composed of compact bone. • 2. The periosteum is a fibrous connective tissue membrane that covers and protects the diaphysis. • 3. Hundreds of connective tissue fibers, called perforating, or Sharpey’s fibers, secure the periosteum to the underlying bone. • 4. The epiphyses are the ends of the long bone, each consisting of a thin layer of compact bone enclosing an area filled with spongy bone.
Structure of Long Bone: • 5. Articular cartilage covers the surface of the epiphyses. Articular cartilage is glassy, hyaline cartilage which provides a smooth, slippery surface that decreases friction at joint surfaces. • 6. The epiphyseal line is a thing line of bony tissue in adult bones spanning the epiphysis that looks different from the bone in that area. • 7. The epiphyseal line is a remnant of the epiphyseal plate (a flat plate of hyaline cartilage) seen in young, growing bone. • 8. In adults, the cavity of the shaft is primarily a storage are for fat (adipose) tissue and is called yellow marrow or medullary, cavity.
Structure of Long Bone: • 9. In infants, the cavity of the shaft forms red blood cells and red marrow is found there. • 10. Bones are covered with bone markings that reveal where muscles, tendons, and ligaments were attached and where blood vessels and nerves passed. • 11. There are two categories of bone markings: • 1) Projections, or processes which grow out from the bone surface • 2) depressions, or cavities, which are indentations in the bone.
Microscopic Anatomy: • 1. Osteocytes are mature bone cells and are found in tiny cavities within the matrix called lacunae. • 2. The lacunae are arranged in concentric circles called lamellae around central Haversian canals. • 3. Each complex consisting of central canal and matrix rings is called an osteon, or Haversian system.
Microscopic anatomy: • 4. Tiny canals, canaliculi, radiate outward from the central canals to all lacunae. • Because of this elaborate network of canals, bone cells are well nourished in spite of the hardness of the matrix, and bone injuries heal quickly and well. • 5. The communication pathway from the outside of the bone to its interior (and the central canals) is completed by perforating (Volkmann’s) canals, which run into the compact bone at right angles to the shaft.
Bone formation, Growth, and Remodeling: • 1) Ossification is the process of bone formation and involves two major phases: • A) The hyaline cartilage model is completely covered with a bone matrix by bone-forming cells called osteoblasts. • So, for a time during fetal development, the fetus as cartilage “bones” enclosed by “bony” bones. • B) Then, the enclosed hyaline cartilage model is digested away, opening up a medullary cavity within the newly formed bone.
Bone formation, Growth, and Remodeling: • 2) By birth, most hyaline cartilage models have converted to bone except two regions: • A) the articular cartilages (that cover the bone ends) • B) the epiphyseal plates • The articular cartilage remain for life resisting friction at the joint surfaces. • The epiphyseal plates provide for longitudinal growth of the long bones during childhood.
Bone formation, Growth, and Remodeling: • As new cartilage is continuously being formed on the external surface of the articular cartilage and epiphyseal plate, the old cartilage that is on the inside of the articular cartilage and the medullary cavity is broken down and replaced by bony matrix. • Growing bones must widen as they lengthen as well. This process is done by the osteoblasts in the periosteum when they add bone tissue to the external face of the diaphysis as osteoclasts in the endosteum remove bone from the inner face of diaphysis wall.
Bone formation, Growth, and Remodeling: • Since the process of bony formation and bone widening happens at the same rate, the circumference of the long bones expands, and the bones widen. • 3) The process by which bones widen is called appositional growth. • This process is controlled by hormones , the most important being growth hormone and, during puberty, the sex hormones. • It ends during adolescence when the epiphyseal plates are completely converted to bone.
Bone formation, Growth, and Remodeling: • 4) Bones are remodeled continually in response to changes in two factors: • a) Calcium levels in blood • b) the pull of gravity and muscles on the skeleton. • How these factors influence bone remodeling involves a number of things.
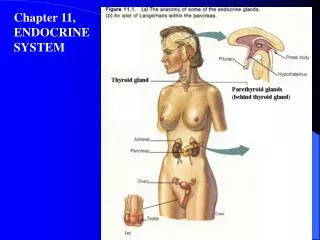
Bone formation, Growth, and Remodeling: • 5) When blood calcium levels drop below homeostatic levels, the parathyroid glands (in your throat) are stimulated to release parathyroid hormone (PTH) into the blood. • 6) PTH activate osteoclasts, giant bone-destroying cells in bones, to break down bone matrix and release calcium ions into the blood. • When blood calcium levels are too high, (hypercalcemia), calcium is deposited in bone matrix as hard calcium salts.
Bone formation, Growth, and Remodeling: • 7) Bone remodeling is essential if bones are to regain their normal proportions and strength during long-bone growth as the body increases in size and weight. • Bones also become thicker and form large projections to increase their strength in areas where bulky muscles are attached. • At these sites, osteoblasts lay down new matrix and become trapped within it, and once they are trapped they become osteocytes, or mature bone cells. • The bones of people who are bedridden or inactive, tend to lose mass and to atrophy because they are no longer subjected to stress. • 8) PTH is the ultimate determinant of when (or if) bone is to be broken down or formed in response to the need for more or fewer calcium ions in the blood.
Homeostatic Imbalance: • Rickets is a disease of children in which the bones fail to calcify. • As a results, the bones soften and a definite bowing of the weight-bearing bones of the legs occurs. • Rickets is usually due to a lack of calcium in the diet or a lack of vitamin D, which is needed to absorb the calcium in the bloodstream. • Rickets is not usually seen in the US where we put such an emphasis on nutrition.
Bone Fractures: • 1. Despite the remarkable strength of our bones, they are subject to fractures, or breaks all throughout our lives. • Fractures are usually the cause of exceptional trauma caused by sports or other injuries. • 2. A fracture in which the bone breaks cleanly but does not penetrate the skin is a closed (or simple) fracture. • 3. When the broken end protrudes through the skin, the fracture is open, or compound.
Bone Fractures: • 4. A fracture is treated by reduction, which is the realignment of the broken bone ends. • In closed reductions, the broken ends are coaxed back into position by the physicians hands. • In open reductions, surgery is performed and the bone ends are secured together with pins or wires. • After the broken bone is reduced, it is held into place by a cast or traction to allow the healing process to begin. • Healing time of a closed fracture is 6-8 weeks, but is much longer in larger bones and bones of the elderly due to poor circulation.
Bone Fractures: • 5. The repair of bone fractures involves 4 major events: • A) A hematoma is formed: Blood vessels are ruptured when the bone breaks. As a result, a blood-filled swelling called a hematoma forms. Bone cells deprived of nutrition die. • B) The break splinted by a fibrocartilage callus: As we learned about in chapter 3, the first step in tissue repair is the growth of new capillaries into the clotted blood at the site of the damage, and the disposal of dead tissue by phagocytes. As this goes on, connective tissue cells of various types form a mass of repair tissue, the fibrocartilage callus.
Bone Fractures: • C) The bony callus is formed: As more osteoblasts and osteoclasts migrate into the area and multiply, the fibrocartilage callus is gradually replaced by one made of spongy bone, the bony callus. • D) Bone remodeling occurs: Over the next few weeks to months depending on the bone size and the site of the break, the bony callus is remodeled in response to the mechanical stresses placed on it, so that it forms a strong permanent “patch” at the fracture site.
The Axial Skeleton: • The axial skeleton forms the longitudinal axis of the body and can be divided into three parts: • 1) The skull • 2) The vertebral column • 3) bony thorax
The Skull: • The skull is formed by two sets of bones: • 1) The cranium encloses and protects the fragile brain tissue. • 2) The facial bones hold the eyes in an anterior position and allow the facial muscles to show our feelings through smiles or frowns. • All but one of the bones of the skull are joined together by sutures, which are interlocking, immovable joints. • Only the mandible (jawbone) is attached to the rest of the skull by a freely moveable joint.
Cranium: • The boxlike cranium is composed of eight large, flat bones except for two paired bones (the parietal and temporal), they are all single bones. • 1) The Frontal Bone: The forehead, the bony projections under the eyebrows, and the superior part of each eye’s orbit. • 2) Parietal Bones: the paired parietal bones form most of the superior and lateral walls of the cranium. • A) They meet in the midline of the skull at the sagittal suture and form the coronal suture where they meet the frontal bone. • 3) Temporal Bones: The temporal bones lie inferior to the parietal bones; they join them at the squamous sutures.
Cranium: • Several important bone markings appear on temporal bone: • a) External acoustic (auditory) meatus is a canal that leads to the eardrum and middle ear. • b) Styloid Process is a sharp, needlike projection, just inferior to the external auditory meatus. Many neck muscles use the Styloid process as an attachment point. • c) Zygomatic Process: is a thin bridge of bone that joins the cheek bone (zygomatic bone) anteriorly.
Cranium: • d) The mastoid process is a rough projection posterior and inferior to the external acoustic meatus, which is full of air cavities (mastoid sinuses). • The mastoid sinuses are so close to the middle ear – a high risk spot for infections – that they may become infected too, a condition called mastoiditis. • Also, this area is so closed to the brain, mastoiditis may spread to the brain itself.
Cranium: • e) Jugular foramen: at the junction of the occipital and temporal bones, and allows passage of the jugular vein, the largest vein of the head, which drains the brain. • f) Just anterior to the cranial cavity is the internal acoustic meatus, which transmits cranial nerves VII and VIII . • g) Anterior to the jugular foramen on the skull’s inferior aspect is the carotid canal, through which the internal carotid artery runs, supplying blood to most of the brain.
Cranium, Occipital Bone: • 4) Occipital Bone: The most posterior bone of the cranium and forms the back wall of the skull. • A) The occipital bone joins the parietal bones anteriorly at the lamboid suture. • B) In the base of the occipital bone is a large opening, the foramen magnum which surrounds the lower part of the brain and allows the spinal cord to connect with the brain. • C) Lateral to the foramen magnum on each side are the occipital condyles which rest on the vetebra of the spinal column.
Sphenoid Bone: • 5) The butterfly shaped sphenoid bone forms part of the floor of the cranial cavity. In the midline of the sphenoid is a small depression, the sellaturcica, or Turke’s saddle, which holds the pituitary gland in place. • A) The foramen ovale, a large oval opening in line with the posterior end of the sellaturcica allows fibers of the cranial nerve V to pass to the chewing muscles of the lower jaw (mandible). • B) Parts of the sphenoid, seen exteriorly forming part of the eye orbits, have two important openings, the optic canal, which allows the optic nerve to pass to the eye, and the slitlike superior orbital fissure through which the cranial nerves controlling eye movements pass. • C) The central part of the sphenoid bone is riddles with air cavities, the sphenoid sinuses.
Ethmoid Bone: • 6) The ethmoid bone is very irregularly shaped and lies anteriorly to the sphenoid. It forms the roof of the nasal cavity and part of the medial walls of the orbits. • A) Projecting from its superior surface is the crista galliin which the outermost covering of the brain attaches to. • B) On each side of the crista galli are many small holes called cribiform plates, which allow nerve fibers carrying impulses from the olfactory (smell) receptors of the nose to reach the brain. • C) Extensions of the ethmoid bone, the superior and middle nasal conchae, form part of the lateral walls of the nasal cavity and increase the turbulence of air flowing through the nasal passages.
Facial Bones: • There are fourteen bones that compose the face, and twelve of these are paired. Only the mandible and vomer are single. • 1) The two Maxillae or Maxillary bones fuse to form the upper jaw. • All facial bones except the mandible join the maxillae, therefore they are the main bones of the face. • A) The Maxillae carry the upper teeth in the alveolar margin.
Facial Bones: • B) Extensions of the maxillae called the palatine processes form the anterior palate of the hard palate of the mouth. • C) The maxillae contain sinuses that drain into the nasal passages known as paranasal sinuses, which serve to lighten the skull bones and act to amplify the sound we make as we speak. • 2) The palatine bones lie posterior to the palatine processes of the maxillae and form the posterior part of the hard palate. • Failure of these or the palatine processes to fuse medially results in cleft palate.
Facial Bones: • 3) The zygomatic bones are often referred to as the cheekbones, but they also form a good part of the lateral surface of the eye sockets. • 4) The lacrimal bones are fingernail-size bones forming part of the medial walls of each eye socket. Each has a groove that serves as a passageway for tears. • 5) The nasal bones are small rectangular bones forming the bridge of the nose. • 6) Thevomerbone is a single bone in the medial line of the nasal cavity. • 7) The inferior nasal conchae are thin, curved bones projecting from the lateral walls of the nasal cavity.
Facial Bones: • 8) The mandible is the lower jaw and is the largest and strongest bone of the face. It joins the temporal bones on each side of the face, forming the only freely movable joints in the skull. • A) The lower teeth lie in the alveoli (sockets) in the alveolar margin at the superior edge of the mandibular body.
The hyoid bone: • The hyoid bone is closely related to the mandible and temporal bones. • The hyoid bone is unique in that it is only bone of the body that does not articulate directly with any other bone. Instead, it is suspended in the midneck region about 1 inch above the larynx where it is anchored by ligaments to the stolid process of the temporal bones. • 9) The hyoid bone serves as a movable base for the tongue and an attachment point for the neck muscles that raise and lower the larynx when we swallow and speak.
Fetal Skull: • The skull of an infant is very different from an adult. • The face of an infant is very small compared to the size of the cranium, but the skull as a whole is large compared to the infant’s total body length. • An adult skull is 1/8 the total body length, but a newborn is ¼ their body length. • 1) In a newborn, the skull also has fibrous regions that have yet to be converted to bone called fontanels. The rhythm of the babies heart can be felt in their fontanels. • 2) The fontanels allow the fetal skill to be compressed slightly during birth as well as become flexible to allow the infant’s brain to grow during the later part of pregnancy and early infancy.
Labeling: • Color and label the skull on your worksheet. • Use the colors to help you identify the different parts of the skull. • It is on pages 141-143 in your book. • We will have a quiz tomorrow over the skull.
Vertebral Column (Spine): • 1) The vertebral column or spine, extends from the skull, which it supports, to the pelvis, where it transmits the weight of the body to the lower limbs. • The Spine is formed from 26 irregular bones connected and reinforced by ligaments in such a way that a flexible, curved structure results. • The spinal cord runs through the central cavity of the vertebral column where it is supported and protected.