Spinal Cord Injury & Disorders (SCI/D) Service
350 likes | 523 Vues
Spinal Cord Injury & Disorders (SCI/D) Service. M. Kristi Henzel, MD, PhD Staff Physiatrist, SCI/D Debbie Rovito, APRN, CNS Clinical Nurse Specialist, SCI/D June 21, 2013. VA SCI/D CENTERS.

Spinal Cord Injury & Disorders (SCI/D) Service
E N D
Presentation Transcript
Spinal Cord Injury & Disorders (SCI/D) Service M. Kristi Henzel, MD, PhD Staff Physiatrist, SCI/D Debbie Rovito, APRN, CNS Clinical Nurse Specialist, SCI/D June 21, 2013
VA SCI/D CENTERS • SCI/D includes traumatic and non-traumatic spinal cord injuries, multiple sclerosis (MS) , and amyotrophic lateral sclerosis (ALS) • Comprehensive system of care formalized in 1996 by the VA, that established a “Hub & Spokes System of Care” to provide acute, sub-acute, and life-long care to Veterans with SCI/Disorders
Spinal Cord Injury and Disorders Center Spinal Cord Injury and Disorders Center 23 VA SCI/D Centers serve ~42,000 veterans with SCI/D Puerto Rico
SCI/D CENTERS • Referral base: Local trauma centers/hospitals - Veterans Department of Defense – Active duty Spoke sites - Veterans Local primary care providers including CBOCs • Standards of care: VHA Handbook 1176 CARF (Rehab Accreditation) standards Consortium for Spinal Cord Medicine Clinical Practice Guidelines • Acuity: Acute medical conditions Complications of chronic SCI Respite care Annual evaluations
SCI/D Hubs & Spokes • Each CENTER has inpatient and outpatient services. • SCI/D Centers provide : • Primary care for veterans with SCI/D in the local area • Acute rehabilitation and tertiary care for veterans referred from the Spoke sites • Each SPOKE site provides primary care and outpatient services for veterans with SCI/D.
CLEVELAND SPOKE SITES Also West Virginia, eastern Indiana, northern Kentucky
CLEVELAND SCI/D CENTER • 32 bed inpatient unit • SCI outpatient clinic, home care & telemedicine program • MDs: Physiatry (PM&R, Internal Medicine, Neurology • Interdisciplinary: • Physical Tx -Rehab nursing • Occupational Tx-Recreational Tx • SCI Psychology-Social work • Research: close affiliation with FES & APT Centers
KEY POINTS • Call us early (transfers OR consults) • When admitting an SCI pt through Urgent Care/ED after hours, page the SCI Attending on call if questions. • Pts are admitted to Medicine Service overnights and transferred to SCI Service the next day, IF appropriate from medical acuity standpoint. • Difference between admission to WSCI (6B floor for SCI nursing care) vs. SCI Service (physician management on WSCI). • Nursing acuity must be less frequent than q4hrs on WSCI/6B. • WSCI has no telemetry.
KEY POINTS • Even if the patient needs to stay on medical floor SCI Service will help with: • Prognostication and classification of SCI • Rehabilitation evaluation • Bowel program • Bladder management • Spasticity management • Skin/Wound issues • Respiratory issues • Treatment of Autonomic Dysreflexia
KEY POINTS • Prognostication– determination of functional recovery and rehabilitation potential. • Neurogenic Bowel – bowel care program best started early to avoid constipation, incontinence and skin breakdown. • Neurogenic Bladder – prevention of renal failure, hydronephrosis and skin breakdown due to incontinence. • Pressure Ulcer Prevention/Treatment – mattress type, turning q2h, avoidance of too much moisture. Wound treatments for new or chronic pressure ulcers. • Spasticity- if acutely changed from pt’s baseline, usually something else is wrong! (i.e. UTI, pressure ulcer, etc.)
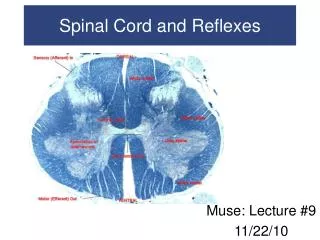
EMERGENCIES IN SPINAL CORD INJURY There are two common SCI emergencies AUTONOMIC DYSREFLEXIA (AD) IS AN ACUTE HYPERTENSIVE EVENT MUCUS PLUGS CAN CAUSE ACUTE RESPIRATORY DISTRESS OR RESPIRATORY FAILURE
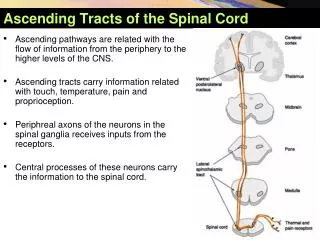
Areas of Autonomic Dysfunction after Spinal Cord Injury • Cardiovascular Function • Respiratory Function • GI function • Lower Urinary Tract Function • Sexual Function • Sudomotor Function • Thermoregulation
AUTONOMIC DYSREFLEXIA • People with SCI who are at risk have injuries at T6 and above. • Noxious stimuli cause unopposed sympathetic reflex activity below the level of injury. • If untreated, acute elevation of BP may lead to stroke, seizures or myocardial infarction
SNS (tonic stimulation) SNS T1-T5 PSNS SNS (~T5-L2)
SNS (tonic stimulation) SCI X SNS T1-T5 PSNS + + + SNS (~T5-L2) + Noxious stimuli from below SCI level + + Increased Afterload vasoconstriction + + + R=8mL/pr4 +
AUTONOMIC DYSREFLEXIA: CAUSES Distended bowel or bladder UTI, Kidney stones Menstruation, pregnancy, labor, delivery Gastric ulcer Sunburn or insect bites Sexual intercourse, ejaculation Scrotal compression DVT and PE Constrictive clothing Ingrown toenail Heterotrophic Ossification, Fractures Infection, Pressure ulcers, Pain
SIGNS AND SYMPTOMS OF AD • Sudden systolic/diastolic BP elevation 20-40 mmHg above baseline. • Individuals with SCI Level of Injury (LOI) above T6 often have baseline SBP’s 90-110. • AD Symptoms: • Bradycardia • Pounding headache • Nasal stuffiness • Profuse sweating usually above the LOI • Goose bumps usually above the LOI • Flushing or blotches usually above the LOI • Blurred vision or spots • Feelings of anxiety • Cardiac arrythmias • AND THEN THERE IS SILENT AD
TREATMENT OF AD • To stop AD you have to identify and remove the cause! • We have a protocol for that! • To order the AD protocol for an at risk patient with SCI go to the SCI Admission Order Set. • With a few clicks you will allow the SCI nurses to start the protocol and safely search for the cause of AD using meds such as lidocaine gel and nitroglycerine ointment. • SCI Nursing will call when they initiate the protocol, and when they need further guidance (usually when they cannot find a cause, or they are really concerned about the patient and his blood pressure).
THE SCI CENTER AD PROTOCOL • Developed from Spinal Cord Consortium CPG & SCI Model Center guidelines and local policy. • Protocol basics CHECK BLOOD PRESSURE + PULSE Q2-5MINUTES SIT THE PATIENT UP / LOOSEN CLOTHING REMOVE SPLINTS + SHOES / CHECK SKIN + TUBES + BODY POSITION CHECK BLADDER / CATHETERS CHECK BOWEL LAST USE MEDS: LIDOCAINE GEL for changing caths or bowel checks NITROPASTE 1 INCH: when BP is above 150
WRAP UP ON AD • AD ends when patient BPs return to baseline. • If the nurse calls you to report all the usual interventions have been tried and BP remains high what should you do? • Even when AD appears resolved, it can reoccur quickly. Nurses will continue to monitor BPs every half hour for two hours after AD ends. • Nurses will put official AD documentation related to their utilization of the protocol in a CPRS Nursing Treatment Note using an Autonomic Dysreflexia template. • At the bedside, the nurses use a worksheet that can guide you, also!
Case Study 54 yo man with C6 tetraplegia is admitted with pneumonia. He is a night float admission to a medical floor but will be transferred to SCI in the morning. At 3AM, the nurse calls to report the patient’s BP is 200/90. His BP was 90/60 when you admitted him. • What do you ask the nurse to do? • Once you open CPRS what do you do? • Who do you call next?
Case Study 54 yo man with C6 tetraplegia is admitted with pneumonia. He is a night float admission to a medical floor but will be transferred to SCI in the morning. At 3AM, the nurse calls to report the patient’s BP is 200/90. His BP was 90/60 when you admitted him. • What do you ask the nurse to do? • Once you open CPRS what do you do? • Who do you call next? By the time you arrive to see how things are going, the early interventions have been done and it was found that the patient was turned on top of his Foley tubing. Once repositioned the bag filled with 600ml of urine and his blood pressure lowered to 90/60
Somatic Innervations of the Respiratory System • The main respiratory muscles are the diaphragm, intercostals and abdominals. • C1-2 SCI: diaphragm is paralyzed and ventilator is required to sustain life. • C3–5 SCI: diaphragm is partially denervated affecting inspiration. C4–C5 SCI do not require ventilation • C6-8 SCI: Primary inspiratory muscles are preserved, but inspiration and expiration impaired, • T1-12: Denervatedintercostal Muscles affecting expiration >> inspiration. • T7-L2 SCI: Denervated abdominal muscles causing ineffective cough.
Respiratory Dysfunction following SCI • Pneumonia • Atelectasis • Bronchitis • Restrictive Airway Syndrome • Sleep Apnea • Respiratory Insufficiency • Dyspnea on Exertion • Leading Cause of Death
MUCUS PLUGS • Mucus plugging may present with acute dyspnea. • Patient may be misdiagnosed with pulmonary embolism or pneumonia • Aggressive pulmonary toilet by RT is essential to assist with removing mucus plugs • Chest vest • Metanebs (Continuous High Frequency Oscillation with positive pressure pulses OR Continuous Positive Expiratory Pressure +/- nebulized medications) • Mechanical In/Ex-sufflation (“Coughalator”) • Keep in mind that some high tetraplegics can quickly experience respiratory failure due to aging, use of opioids, and URIs. • Many individuals with SCI also have OSA.