Understanding Psychosocial Factors in Pediatric Obesity: Counseling Strategies for Families
Pediatric obesity is a growing epidemic, with over 11% of children and adolescents currently classified as obese. This presentation explores the psychosocial factors contributing to obesity in youth and highlights effective counseling strategies for supporting overweight families in clinical settings. By examining key statistics, risk factors, and ethnic disparities, this session aims to equip health professionals with tools to address pediatric obesity in a compassionate and informed manner. Together, we can promote healthier lifestyles and improve the well-being of our children.

Understanding Psychosocial Factors in Pediatric Obesity: Counseling Strategies for Families
E N D
Presentation Transcript
Psychosocial Factors in Pediatric Obesity: Counseling Overweight Youth and Families in your OfficeCarl P. McKnight, Psy.D.Specialized Foster Care Program Los Angeles County Department of Mental HealthOctober 3, 2007
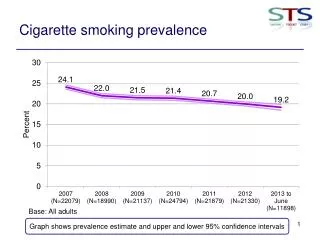
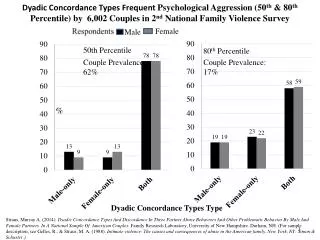
Prevalence • 11% of children and adolescents are currently obese (National Health and Nutrition Examination Survey, 2001) • 22% of children and adolescents are obese, overweight, or at risk to be overweight (Troiano & Flegal, 1998)
Percent Overweight Children U.S. & Orange County Percent Overweight (>95% weight/height) Year Data from the CDC & Prevention, NCHS, NHANES, HHNES, NHES, Report on the Conditions of Children in Orange County, 2002
Percent Overweight 10-12 year olds in Orange County by Ethnicity Percent overweight (>95% BMI) Year Data from the, Report on the Conditions of Children in Orange County, 2002
Percent Overweight 5-9 year olds in Orange County by Ethnicity Percent overweight (>95% BMI) Year Data from the, Report on the Conditions of Children in Orange County, 2002
Childhood Overweight 2003 BMI (Body Mass Index) is Now Defining Tool • BMI Calculated as • Weight / Height Squared • Used to judge appropriateness • of weight for height • Replaces weight for height • charts and % ideal body wt • For a child, BMI > 95% is obese • BMI 85-95% is “at risk” • BMI data from retrospective analysis: • 1. Reflect increasing fatness • 2. Predict adult risk
BMIAdult to Child Predictive Value (NEJM 337:869) Obese AdultsObese Children 15%obese at age6 months 40%obese at age7 years 70% obese at age 12 years 80%obese asadolescents
Epidemic Overweight • 1/4 California children ages 9-17 now overweight (i.e. BMI > 95%) • Fattestkids getting fatter - now twice as many children > 100 lbs overweight as in 1980 • African American, Latino and low socioeconomic children more severely affected (1/3 overweight)
Latinos and Pediatric Obesity • Mexican-American children ages 6-11 are more likely to be overweight (22%) than non- Hispanic children. • Mexican-American adolescents ages12-19 are also more likely to be overwieght (23% of total population).
Latinos and Pediatic Obesity • The higher rates in Latino children start at 6-7 years of age, continue throughout adolescence, and extend into adulthood • Type II diabetes is 2 to 3 times higher in Latino children than in non-Hispanic Whites.
Latinos and Pediatric Obesity • 60% of Latino children and adolescents with Type II diabetes have 1st or 2nd degree relatives with T2DM . • T2DM very common in Mexican-American youths from low income families and is often undiagnosed.
ConsequencesChildhood Obesity It begins… • More than just adult obesity • Adult type diabetes (insulin resistance) • Tall stature • Early puberty • High blood pressure, heart disease • Orthopedic stress and injury (70% of SCFE) • Hyperlipidemia • Sleep apnea & breathing problems • Polycystic ovarian disease • Cancer of endometrium, breast, colon • Gallstones (33% of child cases are obese) • Steatohepatitis (50% of childhood cases) • Emotional and lifecourse disturbances
DM2 in Kids • The Orange County Register May 19, 2003 • Karina Oyarce • 13-years-old Latina in 7th grade • Diagnosed with DM2 in January 2003 • Weighs 200 lbs
Cardiovascular Complications of Obesity • Cardiovascular Disease • Atherosclerosis • Hypertension
Obesity, Hypertension, and Dyslipdemia • Obese children are at a 3 fold higher risk for hypertension than non obese • The risk of hypertension increases with increasing BMI • Dyslipidemia • Overweight Children 2 ½ more likely to have elevated cholesterol • Total cholesterol (TC) >200 • LDL > 130 • HDL<35
Pulmonary Consequences of Childhood Obesity • Decrease in pulmonary function of >15% in >80% of obese children vs. 40% of non-obese children • Obstructive Sleep Apnea: • Abnormal sleep patterns in 94% of obese children • Severe sleep apnea results in hypoventilation, right ventricular hypertrophy & heart failure, possible pulmonary embolisms
Summary Childhood Obesity Risk FactorsUSA Today Survey 1. Too much milk in infancy 2. Too much soda 3. Too much juice 4. Use / overuse of ketchup (or ranch dressing) 5. Eating in front of the TV 6. Watching more than 2 hours per day of TV 7. Eating from snack machines 8. Eating in the car 9. Skipping breakfast 10. Not participating in PE
Variables Contributing to the Development of Obesity • NATURE verses NURTURE • Familial Variables/Genetics • general consensus regarding genetic link in developing obesity (Myer & Stukard, 1993) • Familial Variables/Shared Environment • For infants/young children, parents play a central role in providing food and activity choices in the household • Can influence regulation of hunger and satiety cues
Variables Contributing to the Development of Obesity • Toxic Environment in America • decreased access to physical activity • increased sedentary activities • increased access to high-fat and high calorie foods
Psychological Assessment • Psychosocial Correlates • “Being overweight during childhood and adolescence is potentially associated with a number of negative psychosocial outcomes” (Jelalian & Mehlenbeck, 2003, p. 530). • Social problems & deficits • Depression • BMI positively correlated with depressive symptoms in girls (Erickson, Robinson, Haydel, & Killen, 2000)
Five Warning Signs of Depression • 1) Sad anxious or “empty” mood • “Have you felt sad/ worried or just not like yourself lately?” • 2) Declining school performance • “Have you noticed that school is harder for you than it used to be, or that you are not doing as well as you used to?” • 3) Loss of pleasure/interest in social and/or sports activities • “Do you find that you do not enjoy activities as much as you used to?” • 4) Sleeping too little or too much. • “Are you finding that you are sleeping a lot more or a lot less than you used to?” • 5) Changes in weight or appetite • “Has your appetite changed lately?”
Psychological Assessment • Self-esteem • low views of physical and general self worth (Braet, Mervielde, & Vandereycken, 1997) • self esteem decreases between school age and adolescence (Strauss, 2000). • diminished self-efficacy with respect to physical activity (Trost, Kerr, Ward, & Pate, 2001) • Quality of life (JAMA, 2003) • obese children’s rated quality of life is as low as pediatric cancer patients
Psychological Assessment • Eating Disorders • Obesity is a major risk factor for the development of eating disorders (Fairburn, Welch, Doll, Davies, & O’Conner, 1997). • Eating Disorder NOS (Binge Eating Disorder) • recurrent episodes of binge eating in the absence of inappropriate compensatory behaviors characteristic of Bulimia Nervosa (DSM-IV; American Psychiatric Association). • Important to rule out Prader-Willi syndrome
Psychological Assessment • Recommendations for taking histories • Assess the following areas: • social functioning • self-concept • mood • eating disorders
Psychological Treatment • Overview. Most interventions with obese children are delivered in a group setting and contain: • 1) Dietary Restriction • 2) Physical Activity Prescription • 3) Behavioral Modification • 4) Parental Involvement
Psychological Treatment • Dietary Interventions • “Traffic Light Diet” (Epstein, Wing , & Valoski, 1985) • RED: limit high fat foods • Y ELLOW: moderate amounts of yellow/starchy food • GREEN: freely eat fruits and vegetables • Physical Activity Interventions • increasing lifestyle physical activity as well as decreasing sedentary behaviors (Epstein, Paluch, Gordy, & Dorn, 2000). • Physical activity that can be incorporated into daily routine • Start with 30 minutes of exercise a week, add 30 minutes each week, with goal of 180 minutes per week.
Psychological Treatment • Behavioral Interventions • self-monitoring dietary intake and physical activity • stimulus control • change the environment to ensure success ( have no sodas in the home) • contingency management (positive reinforcement) • providing rewards for decreases in BMI and sedentary behaviors as well as improvements in diet and exercise.
Setting Goals • Explore the problem • what has or has not worked in past • Determine meaning of problem • feelings,barriers, costs, benefits to change • Identify goals that are realistic • Determine a plan of action • simple, specific, part of routine • Evaluate outcome • modify strategies
Identify goals • Select one or two priority areas that needs to change (ex, long term goal of losing weight) • Decide behavior goals related to above (short term goals) • small change in eating behaviors • small change in exercise • gradually increase expectations with rewards at each step
Practical Recommendations • General Considerations (Jelalian & Mehlenbeck, 2003) • Assess child’s or adolescent’s motivation for weight loss • does child have concerns about weight? • does child get teased? • can child keep up with peers during physical activities with peers? • If motivation mainly from parent, then family interventions are needed • If child is motivated, then can teach how to learn healthier behaviors
Practical Recommendations • Family-Based Interventions • engage entire family • promote idea that healthy habits may benefit all family members • encourage parents to assume responsibility for foods available inside the home • promote activities unrelated to eating to mark special events • do not use food as a reward • encourage parents to monitor frequency of “screen time.”
Practical Recommendations • Kaiser’s Brief Negotiation: Communication Guidelines to Promote Behavior Change • Very helpful tool to briefly assess motivation to change
Stages of Change Model Five stages of change • Precontemplation • Contemplation • Preparation • Action • Maintenance
Precontemplation Stage Not Intending to Change • Doesn’t believe behavior has negative consequences • May be resistant to change • Health professionals may be resistant to intervening with this stage • Cons >> Pros • Self-confidence
Contemplation Stage Intending to Change • Knows the negative consequences • Doesn’t know how to get started • Cons > Pros • Externally motivated • Self-confidence
Preparation Stage Making small/inconsistent changes • Know a little about how to get started • Don’t know how to stay with it; need a plan • Cons = Pros • Externally motivated • Typically the people who participate in “action” programs • Self-confidence
Action Stage Doing the behavior regularly but for < 6 mos. • Greatest risk for relapse • Most use of the processes of change • Cons < Pros • Externally (and internally) motivated • Most likely to participate in “action” programs • Self-confidence
Maintenance Stage Sustaining the change • Continue to do the behavior no matter what • The processes of change are now skills • Cons < < Pros • Internally motivated; part of value system • Self-confidence
Processes of Change Behavioral Strategies (later stages) Making a Commitment Enlisting Social Support Substituting Alternatives Rewarding Yourself Reminding Yourself Information Strategies (earlier stages) Increasing Knowledge Comprehending Benefits Warning of Risks Caring About Consequences Increasing Healthy Opportunities