Understanding Memory: Models, Types, and Neuropsychological Impacts
This overview presents the fundamentals of memory models, distinguishing between declarative (explicit) and procedural (implicit) memory. It delves into the neuropsychological underpinnings of memory, including kindling and sensitization and their connections to memory processes. Key types of memory are explored, including short-term and long-term memory, and the relationship between emotional significance and memory retention. The anatomical structure involved in memory storage, including the role of the hippocampus and the limbic system, is discussed alongside significant case studies, such as Patient H.M., highlighting the complexities of memory formation and recall.

Understanding Memory: Models, Types, and Neuropsychological Impacts
E N D
Presentation Transcript
MEMORY Tim Kimbrell, M.D.
OBJECTIVES • overview of memory models • differences between declarative (explicit) and procedural (implicit) memory • kindling/sensitization and its relationship to memory • neuropsychological basis of memory and common forms of amnesia
OVERVIEW • Changes in neural networks must occur to encode and retrieve information • A memory is access to previously learned information (experience) • Bottom line: Brain function and ultimately Brain structure are changed with experience (learning)
MOTIVATION OR EMOTIONAL MEANING • Classic example of inverted “U” curve applies to memory/learning, cerebral blood flow, performance, etc. (Gur and Gur) • Mild to moderate attention/arousal are necessary • Basic science courses re a marathon, not a sprint • Fear of failure: desire to do your best
DECLARATIVE OR EXPLICIT MEMORY • Conscious or cognitive memory • Distinct facts and your awareness of knowing them (Arkansas won the Cotton Bowl) • All important in Medical School • Key: How long will you remember this stuff?
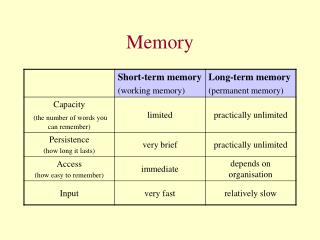
DECLARTAIVE/EXPLICIT MEMORY • SHORT-TERM: SECONDS TO MINUTES • Hear it/see it --think about it • Association cortex -- Prefrontal cortex • Working memory is an example • Ask patient to remember 3 objects
DECLARATIVE/EXPLICIT MEMORY • LONG-TERM: HOURS/DAYS TO A LIFETIME Association Cortex Medical temporal Prefrontal cortex What did you have for breakfast on Tuesday? What year were you married?
PROCEDURAL (IMPLICIT) MEMORY • Knowing how to do things without “thinking” -- swing a golf club, play piano • Storage mechanism: inherent to various sensory and motor areas • Cerebellum/amygdala known to be important
MEMORIES AND CIRCUITS • REVERBERATING MODEL: DYNAMIC IN NATURE • Stimulus enters the pathway and continues to bounce back and forth • Information “burned as a trace into the living” and thus localized • Though discredited, probable role in autobiographical memory
CONVERGENCE MODEL • Convergence of 2 excitatory signals giving change at a synaptic level (plastic) • Similar to post tetanic potentiation • Arousal is accounted for • Localization is not required • Experience changes the anatomy of the brain
APLYSIA STUDIES • Kandel demonstrated plasticity and will win the Nobel Prize • Studied a simple reflex in sea slug • Photographed morphologic change with experience/learning
HABITUATION • Repeated stimulation: attenuated/decreased response • What causes the neuron to fire? • Calcium influx decreases • If not firing, less glutamate needed, decreased mobilization and receptor number
SENSITIZATION • Restoration and potentiation of the response • Apply a noxious stimuli to sensory system • Increase neurotransmitter release • Increase “active zones” at the synapse • Inhibit protein synthesis-- block effect
PLASTICITY Sensory and motor neurons “store” information in a distributed network that is modifiable by experience and results in a change in synaptic strength
LONG TERM POTENTIATION (LTP) • Frequent stimulation/sensory input • Glutamate release and binds to NMDA receptors mediating increase in Calcium influx • Activation of phosphoproteins and transcription pathways change post synaptic structure
LONG TERM DEPRESSION/HABITUATION • Low frequency stimulation over time • Inhibition of “Meaning/significance” • Frequent half-ass attempts are not productive
ANATOMY • All brain regions play a role • Association cortex • Visual/Verbal/olfactory = sensory long term storage • Cerebellum: Procedural and declarative • Frontal cortex: Awareness/Consciousness
LIMBIC SYSTEM • Older, more primitive regions of brain • Grande Lobule Limbique • Emotional significance is contributed • Arousal “system”
LIMBIC SYTEM (continued) • Hippocampus/Amygdala; Cingulum septal region, anterior thalamus orbitofrontal cortex hypothalamus • Emotional significance provides motivation median forebrain bundle/fornix
HIPPOCAMPUS/MEDIAL TEMPORAL Most studied region related to memory • Assimilates short term to long term memory distributes to cortical regions for storage • perfused by end arteries: easily damaged • concentrated Glucocorticoid receptors
KLUVER-BUCY SYNDROME • Primates after undergoing bilateral temporal lobectomy • Hyperorality, hypersexuality and placidity • Amygdala resection necessary for full syndrome • Total amnesia: need bilateral injury to Hippocampus and possibly other medial structures
PATIENT HM • Most famous/studied patient in neurology • Bilateral hippocampal resection • Complete anterograde amnesia • Dominant Hippocampus: Auditory deficits • Non-dominant Hippocampus: Visual deficits • Cueing: make use of what you have
PRIMING • Interface between declarative and procedural • Latency between presentation and identification • HM insisted he hadn’t seen the picture • Retention of procedural memory w/o declarative
PATIENT HM (continued) • Mirror writing improved with practice • Ribot’s Law: oldest memories are most resistant to damage or decay • Natural decay: Review notes intermittently
PHARMACOLOGY • Glutamate : excitatory; make $$$ • Glycine: spinal cord excitation • GABA: inhibitory; benzodiazepine/ETOH • Acetylcholine: Displace Mg ion at NMDA receptor • Avoid anticholinergics in elderly • nucleus basalis
AMNESIA • Specific defect in declarative memory - other functions preserved • Retrograde: Loss of stored memories • Anterograde: Inability to form new memory
ALCOHOLIC BLACKOUTS • ETOH mechanism of action • Sensitization occurs • Cross reactivity with Benzodiazepines • Use long acting agents
WERNICKE-KORSAKOFF’S • Occurs with alcohol dependence • Destruction of mamillary bodies (loop of Papez) • Can be arrested if caught early
SHORT DURATION AMNESIA • Partial complex seizures: episodic • Medial temporal lobe seizure focus • Basilar artery migraines • Origin of posterior cerebral arteries
LONG DURATION AMNESIA • Herpes simplex encephalitis • Attacks medial temporal lobe (anterograde amnesia) • May resemble Kluver-Bucy
PSYCHOGENIC AMNESIA • Fugues and dissociative disorders • Stressor often involved • Most often retrograde in nature • Frequently clears with time • Retains ability to form new memories • “Knuckleheads” need best assessment
ASSESSMENT • Complete history and physical • Keep a wide differential diagnosis • Examine sensory systems • Make use of imaging/EEG