Download
1 / 62
1.94k likes | 5.58k Vues
Nursing Interpretation of the Electrocardiogram (ECG), Telemetry. By: Teresa Champion MCC NURS 2140. OBJECTIVES. Describe the configuration of the normal electrocardiogram (ECG).

E N D
Nursing Interpretation of the Electrocardiogram (ECG), Telemetry By: Teresa Champion MCC NURS 2140
OBJECTIVES • Describe the configuration of the normal electrocardiogram (ECG). • Identify and calculate heart rate, rhythm, PR interval, QRS complex, and QT interval for normal and abnormal cardiac rhythms. • Discuss the etiology and significant ECG features of the following dysrhythmia classifications: sinus, atrial, junctional, block, ventricular, and asystole. • Interpret the significance of each of the dysrhythmias and formulate nursing responsibilities for each dysrhythmia. • Identify normal rhythms and dysrythmias. • Identify ECG complexes and artifact. • Perform ECG rhythm strips. • Identify correct dysrythmia terminology
Cardiac Conduction System • 3 Main Parts: • SA node (Sinoatrial node) • AV node (Atrialventricla node) • HIS-Perkinje System
VIDEO OF CONDUCTION SYSTEM http://www.nhlbi.nih.gov/health/dci/Diseases/hhw/hhw_electrical.html
Anatomy of the Heart - CARDIAC CELLS • Two types of cardiac cells • Myocardial & Pacemaker cells • Automaticity • Excitability • Conductivity • Contractility
Anatomy of Heart – Cardiac Chemistry Function • Electrolytes Affecting Cardiac Function • Depolarization/Repolarization • Cardiac Output (CO): The amount of blood the heart pumps out to body in 1 min. NORMAL: 5 to 8 L • CO= HR x SV (CO can be changed by altering heart rate, stroke vol. or both) • Stroke Volume = the amount of blood that the • heart ejects in one beat which • depends on activity level, physical • condition, prior heart disease
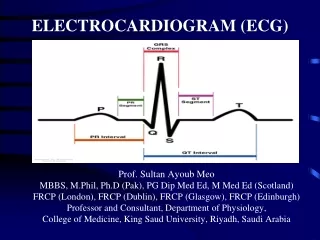
Cardiac Wave Form on Electrocardiogram (ECG) • P wave • PR interval • QRS complex • J point • ST Segment • T wave • QT Interval • R to R Interval • U wave (not always present)
ECG Lead Placement in Telemetry • 1. The white lead is placed on the right side of the chest. This is usually called the “right arm lead.” • 2. The black lead is placed on the left side of the chest. This is called the “left arm lead.” • 3. The green lead is placed on the right lower abdomen, it is called the “right leg lead.” • 4. The red lead is placed on the right lower abdomen, it is called the “left leg lead.” • 5. The brown lead is placed slightly to the right of the midsternum, it is called the “V lead or chest lead.” • 6. The grey lead is
Lead Placement ECG Telemetry White lead Black Lead Brown Lead Green Lead Red Lead
Heart Rate on ECG • Heat Rate • Fastest count R waves in 6 second strip and times by 10. • Count R waves on a full minute strip for accurate HR for irregular rhythms. • Another way is to count the number of small boxes between R waves and divide the total by 1500.
Heart Rate on ECG 1 big box (5 small boxes) is equal to a HR of 300 2 big boxes is hr of 150 (300/2) 3 big boxes is hr of 100 (300/3) 4 big boxes is hr of 75 (300/4) 5 big boxes is hr of 60 (300/5) 6 big boxes is hr of 50 (300/6) 7 big boxes is hr of 43 (300/7) 8 big boxes is hr of 38 (300/8)
A dysrhythmia is a disturbance of the rhythm of the heart caused by a problem in the conduction system. • Categorized by site of origin: atria , AV nodal, ventricular • Blocks are interruptions in impulse conduction: 1st, 2nd type 1&2, 3rd or complete heart block
P wave Measures: 0.12-0.20
QRS WAVE Measures: 0.06-0.10
QT Wave Measures approx 0.36-0.48 seconds
Heart rates • NSR: heart rate is 60-100bpm • ST: heart rate 101-180 bpm • SB: heart rate <60 bpm
Sinus rhythm • PR interval- 0.12-0.20sec • QRS-0.06-0.10sec • QT segment 0.36-0.44 sec • Heart rate 60-100
Atrial arrhythmias • Sinus tachycardia • Atrial tachycardia • Sinus bradycardia • Premature atrial contraction (PAC) • Supraventricular tachycardia • Atrial fibrillation • Atrial flutter
Other Atrial Dysrhymias • Wolf Parkingson-White Syndrome (WPW) • Wandering Atrial Pacemaker (WAP) • Sick Sinus Syndrome (SSS)
Management of Atrial Dysrhymias • Assess pt response/Monitor Vital Signs • May cause drop in Cardiac Output (CO) • Notify MD (Health Care Practitioner) • Intervention to convert back to NSR • Increase rate – slow rates, Administer drugs (Atropine), Transcutaneous Pacing • Control rate – if fast Ventricular Response (ie: A-fib, SVT, Aflutter) • Anticoagulate • Cardioversion
How to treat SVT • B-blockers ( to decrease conduction thru AV • node: • Calcium channel blockers ( to decrease conduction • thru AV node) • Radio frequency ablation • SVT converted with Adenosinegiven rapid IV Push stimulates vagal response.
Atrial Fibrillation • - - 5 to 6 times more likely to have stroke • - - atrial rate: 300 to 600 times/minute • --prolonged A-Fib may stretch & weaken • heart muscle • - - symptoms: lightheaded, very tired, • SOB, diaphoretic, chest • pain,
A Fib electrical cardioversion: • High risk of forming clots & causing stroke • Anticoagulants taken before treatment and 3-4 weeks post treatment • If life-threatening, may need Heparin IV before cardioversion • Best time: recent A fib
Ventricular arrythmias • Junctional rhythms • AV blocks • Premature ventricular contraction (PVC) • Ventricular Tachycardia (V-tach) • Ventricular Fibrillation (V-Fib) • Torsade de Pointes (TdP) • Pulseless electrical activity (PEA) • Asystole
AV Blocks • First degree block • Second degree block Type I (Wenchebach) • Second degree block Type II (Mobitz II) • Third degree block • Bundle branch block
First degree heart block Rate is usually WNL Rhythm is regular Pwaves are normal in size and shape The PR interval is prolonged (>0.20 sec) but constant
Second degree heart block type 1 (Mobitz I or Wenchebach) Pwaves are normal in size and shape; Some pwaves are not followed by QRS PR interval: lengthens with each cycle until it appears without QRS Complex then the cycle starts over QRS is usually narrow
Second degree heart block type 2 (Mobitz II) • Ventricular rate is usually slow • Rhythm is irregular • Pwaves are normal in size and shape (more pwaves than QRS) • PR interval is within normal limits • QRS is usually wide
3rd degree heart block or complete heart block • Ventricular rate is regular but there is no correlation between p-waves and QRS • P waves are normal in size and shape • No true PR interval
PVC Unifocal Multifocal
PVC: ventricular origin • Complex is wide followed by compensatory pause • An irritable focus in ventricle initiates a contraction before normally expected beat. • Acute MI most common cause • QRS is wide and bizarre • Risks: increasing myocardial irritability, leading to increased freq. of PVCs • Can occur as bigeminy (every other beat) • or short runs
Ventricular tachycardia Monomorphic: beats are same size and shape Polymorphic: different size and shape
Torsades de pointe This is a polymorphic VT Usually electrical imbalance in r/t NA+ or K+
V-tach • Advanced irritability of ventricles due to ASHD, CHF, acute MI electrolyte imbalance. Hypoxia, acidosis, occasionally drugs • RISKS: low to no Cardiac output • Nursing Interventions: monitor, if pt unconscious, immediately defibrillate