Download

1 / 58
600 likes | 1.26k Vues
Chapter 14: The Kidneys and Regulation of Water and Inorganic Ions. Section A: Basic Principles of Renal Physiology : 1- Glomerular filtration 2- Tubular reabsorption 3- Tubular secretion. Figure 14-1.

E N D
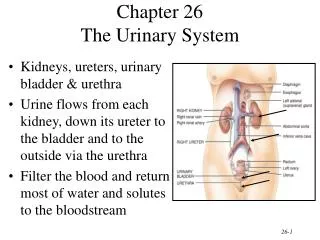
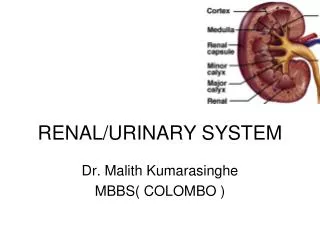
Chapter 14: The Kidneys and Regulation of Water and Inorganic Ions
Section A: Basic Principles of Renal Physiology: 1- Glomerular filtration 2- Tubular reabsorption 3- Tubular secretion
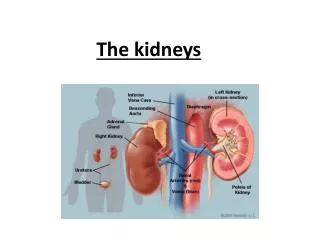
Figure 14-1 The paired kidneys form a filtrate of the blood that is modified by reabsorption and secretion; urine designated for excretion moves along the ureters to the bladder.
Figure 14-2 Fluid filtered from the blood in the glomerular capillaries is altered by reabsorption and secretion along the length of the 1,000,000 nephrons/kidney.
Figure 14-3 Due to the hydrostatic pressure of the cardiac pump, fluid is filtered from the blood through fenestra in the glomerular capillaries into slit pores in the capsule.
Figure 14-4 The outer layer of the kidney is the renal cortex; it is the site of glomerular filtration and the convoluted tubules. The inner part of the kidney is the renal medulla; this is the location of the longer loops of Henle, and the drainage of the collecting ducts into the renal pelvis and ureter.
Figure 14-5 The intersection of the macula densa in the distal tubule with the afferent and efferent arterioles forms the juxtaglomerular apparatus, which secretes the endocrine signal known as renin into blood in the afferent arteriole.
1. Glomerular filtration refers to the movement of fluid and solutes from the glomerular capillaries into Bowman’s space. Figure 14-6
1. Glomerular filtration refers to the movement of fluid and solutes from the glomerular capillaries into Bowman’s space. 2. Tubular secretion refers to the secretion of solutes from the peritubular capillaries into the tubules. Figure 14-6
1. Glomerular filtration refers to the movement of fluid and solutes from the glomerular capillaries into Bowman’s space. 2. Tubular secretion refers to the secretion of solutes from the peritubular capillaries into the tubules. 3. Tubular reabsorption refers to the movement of materials from the filtrate in the tubules into the peritubular capillaries. Figure 14-6
Figure 14-7 Substance X is filtered and secreted but not reabsorbed. Substance Y is filtered and some of it is reabsorbed. Substance Z is filtered and completely reabsorbed.
Figure 14-8 Formation of the glomerular filtrate in Bowman’s capsule is the outcome of opposing pressures: hydrostatic pressure from the heart favors filtration, osmotic and hydrostatic pressure of the filtrate oppose it.
Figure 14-9 As vasodilation and vasoconstriction of the afferent and efferent arterioles alter the blood flow through the glomerular capillaries, there are corresponding alterations in the glomerular filtration rate (GFR).
Figure 14-10 The luminal section of the plasma membrane of the tubule cells faces the filtrate, whereas the basolateral section is in close proximity to the peritubular capillary.
Figure 14-11 Inulin, a biologically inert polysaccharide, can be used to estimate the glomerular filtration rate since it is filtered, but not reaborbed or secreted.
Figure 14-12 Release of urine from the bladder, called micturition, is coordinated by a combination of smooth and skeletal muscle relaxation and contraction.
Section B: Regulation of Sodium, Water, and Potassium Balance:
An consuming ion pump in the basolateral membrane of the collecting duct cell moves Na+ toward the blood in the peritubular capillary . . . ATP Peritubular capillary to bladder Figure 14-13
An ATP-consuming ion pump in the basolateral membrane of the collecting duct cell moves Na+ toward the blood in the peritubular capillary as it produces the gradient that facilitates Na+ entry across the luminal section of the cell . . . Peritubular capillary to bladder Figure 14-13
An ATP-consuming ion pump in the basolateral membrane of the collecting duct cell moves Na+ toward the blood in the peritubular capillary as it produces the gradient that facilitates Na+ entry across the luminal section of the cell; K+ movements are in the opposite direction. Peritubular capillary to bladder Figure 14-13
Figure 14-14 When membranes are permeable to water molecules, osmosis drives them to follow the movement of sodium ions pumped across membranes by the ion pumps. Water can also diffuse through adjacent tubule cells. Sodium pumping thus accomplishes water reabsorption.
Figure 14-15 The renal counter-current multiplier system establishes the osmotic gradient required for the formation of hyperosmotic urine.
Figure 14-16 The geometry of the vasa recta parallels the renal counter-current multiplier system, assuring that the blood in these vessels does not “wash out” the osmotic gradient.
Figure 14-18 Alterations in GFR are mediated by a variety of neural and endocrine factors, and constitute a major influence on the amount of water lost from the body in urine.
Figure 14-19 The “ACE” system is initiated by abnormally low pressure in the renal blood supply, or by other factors that cause renin secretion from the juxtaglomerular cells. Renin activates the formation of angiotensin I, which is converted to angiotensin II by Angiotensin Converting Enzyme (ACE). Angiotensin II is a vasoconstrictor (reduces GFR) and promotes the synthesis of aldosterone, an adrenal steroid hormone that increases sodium and water reabsorption in the distal tubules.
Figure 14-20 The varied pathways to increased renin secretion are illustrated in this chart, as are the subsequent steps leading to increased levels of angiotensin II in the blood. Note that the vasoconstrictor action of angiotensin II allows it to decrease GFR as a direct result of decreasing blood flow through the glomerular capillaries.
Figure 14-21 An abnormal increase in blood volume “stretches out” the atria, stimulating secretion of ANP (atrial natriuretic peptide). ANP promotes vasodilation, thus increasing GFR, and inhibits sodium reabsorption in the distal tubule, leading to natriuresis (increased levels of sodium in urine), which increases urine volume as it decreases blood volume. & water
Figure 14-22 An abnormal decrease in blood volume and pressure activates baroreceptor neurons in the aorta and carotid sinuses, leading to increased secretion of vasopressin, also known as anti-diuretic hormone (ADH); which increases water permeability in the collecting ducts, which decreases the volume of excreted urine.
Figure 14-23 Drinking too much water causes an abnormal decrease in fluid osmolarity, which alters the activity of hypothalamic osmoreceptors, which then reduces activity of ADH neurons, leading to decreased secretion of ADH; water permeability in the collecting ducts is reduced, thus increasing the volume of excreted urine, a condition called diuresis.
Figure 14-24 Severe loss of body water decreases GFR and increases levels of aldosterone, vasopressin, and angiotensin II (not shown); these adaptive responses act to promote water conservation in the renal system to help restore blood volume and pressure.
Figure 14-25 The diversity and redundancy of signals that alter water appetite, also known as “thirst,” demonstrate the importance and adaptive value of the homeostatic maintenance of blood volume and pressure.
Figure 14-26 Potassium is filtered from the glomerular capillaries. The relative rates of potassium reabsorption and secretion are determined by the law of mass action and by aldosterone, which increases sodium reabsorption at the “expense” of increased potassium secretion.
Figure 14-27 Ingesting too much potassium stimulates aldosterone secretion from the adrenal cortex; aldosterone increases sodium reabsorption at the “expense” of increased potassium secretion. Also shown here is an indication that more potassium in the filtrate leads to greater potassium excretion in the urine.
Figure 14-28 Decreased blood volume and ingesting too much potassium both stimulate aldosterone secretion from the adrenal cortex; aldosterone increases sodium reabsorption at the “expense” of increased potassium secretion.
Section C: Calcium Regulation:
Figure 14-29 Osteoblasts build bone. Osteoclasts catalyze bone degradation, when stimulated by parathormone (PTH).
Figure 14-30 The four parathyroid glands are located adjacent to the much larger thyroid gland. Secretion of parathormone (PTH) is a direct response to an abnormal decrease in the concentration of calcium ions.
Figure 14-31 Parathormone’s action to restore normal calcium levels include increased calcium reabsorption in the kidneys, increased calcium-liberating activities of osteoclasts, and increased formation of vitamin D, which increases uptake of dietary calcium in the gastrointestinal tract.
Figure 14-32 Activated 1,25 (OH)2D3 is a steroid hormone that causes cells in the gut to increase the expression of genes whose products take up dietary calcium.
Section D: Hydrogen Ion Regulation: