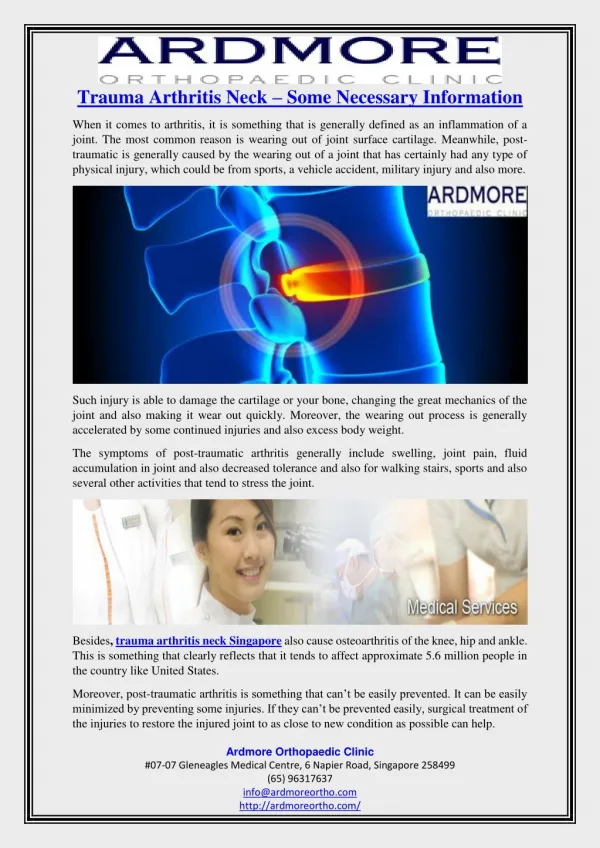
Neck Trauma
Neck Trauma. Presented by: Rauchel R. Lyons, RN. Student Learning Objectives. Identify the common organ structure involvement. Identify neck w ound location classification by anatomic zones. Recognize hard and soft signs of Arterial bleeding. Approach to Neck Trauma.


Neck Trauma
E N D
Presentation Transcript
Neck Trauma Presented by: Rauchel R. Lyons, RN
Student Learning Objectives • Identify the common organ structure involvement. • Identify neck wound location classification by anatomic zones. • Recognize hard and soft signs of Arterial bleeding.
Approach to Neck Trauma • Involves multitude of organ systems (example: airway, vascular, neurological, and gastrointestinal) and structures (example: musculoskeletal, neural, vascular, visceral, and glandular. • Airway occlusion and exsanguinating hemorrhage is most life threatening. • Wounds may be overlooked and may not manifest clear signs and symptoms
Types of Neck Trauma • Penetrating trauma • Blunt trauma
PATHOPHYSIOLOGY • Mechanism of injury • Stab Wounds • Motor vehicle • Household Injuries • Industrial Accident • Sporting Events
Organ System Involvement • Vascular (most common) • Pharyngoesophageal • Rarely causes any immediate consequence. • Delayed diagnosis can lead to serious soft tissue infection, mediastinitis and sepsis. • Laryngotracheal • Small puncture wound • Airflow away from respiratory tree • Obstruction of airway • Others (cranial nerve, thoracic duct, brachial plexus, spinal cord….)
Vascular • Three Pathophysiological Mechanisms • External hemorrhage • Extending soft tissue hematoma, distort or obstruct the airway • Disruption of cerebral perfusion
Wound Location Classification by Anatomical Zones • Anterior and Posterior (Sternocleidomastoid muscle separating) • Anterior • Zone 1 (below cricoid cartilage) • Zone 2 (between the cricoid cartilage and mandible angle) • Zone 3 (above mandible angle)
Management of Penetrating Trauma • Stabilization • Critically injured patient • Rapidly assessing vital functions and the area of injury • Performing stabilizing interventions • Initiating a diagnostic workup • No immediate life threat • Violates the platysmal muscle (explore at operating room) • If hemodynamic stability cannot be achieved, prompt transfer to the operating room is in order
Assessment • Inspect • Airway • Respiratory distress • Platsymal muscle breech (any breech is potential for grave damage to the contents of the neck) • Air bubbling through wound • Hemoptysis or blood - tinged saliva • Shock or active bleeding • Arterial injury • Gross bleeding or presence of a hematoma
Hard and Soft Signs of Arterial Injury • Hard • Large expanding hematoma • Severe active or pulsatile bleeding • Shock unresponsive to fluid intervention • Signs of cerebral infarction • Presence of bruit or thrill • Diminished pulses • Soft • Nonexpanding hematoma and paresthesias that does not improve.
Assessment • Palpate • Pulses distal to injury • Subcutaneous emphysema • Unnecessary probing or manipulation of the wound or performing any action that may cause the patient to cough, gag, or choke is discourage for it may dislodge a clot and pose life threatening.
Interventions • External Hemorrhage • Direct pressure or balloon tampanade • Place in mild Trendelenberg to decrease air embolism risk • Do not blindly clamp transected vessel • Do not remove object • Rapid transfer to the operating room • Internal Hemorrhage • Prepare for intubation if airway compromised • Prepare for thoracostomy if Zone 1 injury resulting in hemothorax
Management of Penetrating Neck Trauma • Unstable patient • Immediate transfer to the operating room • Stable patient • General • Mandatory exploration • Selective Approach
Definitive Management of Penetrating Neck Trauma Stable • General • Standard trauma blood studies • Lateral neck film • Chest radiography (especially in zone 1 injuries ) • Nasogastric tube should not be inserted • Prophylactic antibiotics • Mandatory exploration • Selective Approach • A selective method reserves operative intervention for patients with clinical signs of significant injury
Other Diagnostic Studies • Bronchoscopy • Esophagography • Esophagoscopy • Angiography Patients with Zone 2 wounds who have no clinical manifestation of vascular injury are believed to require no vascular studies
Blunt Neck Trauma • Rare, compared with penetrating trauma • Spinal column and spinal cord injuries are more prevalent in blunt trauma
Mechanism of Injury • Motor vehicle crashes • Sports related injury (clothesline tackle) • Strangulation & near hanging • Blows from the fists or feet • Excessive manipulation (example chiropractic treatment) • Iatrogenic
Organ System Involvement • Vascular : delayed dissection or thrombosis • Laryngotracheal • Pharyngoesophageal
Four Recognized Mechanisms by Which Thrombosis Can Occur • A direct blow to the neck • Hyperextension and/or rotation of the head and lateral neck flexion resulting in a stretch injury to the vessels • Blunt intraoral trauma • Basilar skull fracture
AssessmenT Physical findings may be lacking , it is important to elicit symptoms • Aerodigestive Tract Disruption • Dysphagia • Voice quality • hoarseness • Dysphonia • Dyspnea
Management of Blunt Neck Trauma • Laryngeal injuries do not require immediate repair • Tracheal injuries should receive prompt surgical attention
Definitive Management • General • Standard trauma blood studies • Cervical spine radiography • Chest radiography • Additional Studies • Computed Tomography Scan • Endoscopy (fiberoptic bronchoscopy ) • (Consult chest surgeon or Ear Nose and Throat surgeon) • Angiography • Color Flow Doppler ultrasound • Esophageal & esophagoscope • (Consult chest surgeon)
Specific Signs Related to Injury to Specific Structures • Larynx or tracheal • Penetrating the heart, aorta, and great vessels • Tracheobronchial or lung • Carotid artery • Jugular vein • Esophagus and pharynx • Spinal Cord • Cranial nerve
Larynx or tracheal injury • Voice alteration • Hemoptysis • Stridor • Drooling • Sucking, hissing, or air frothing or bubbling through the neck wound (It may be provoked by coughing.) • Subcutaneous emphysema and/or crepitus • Hoarseness • Dyspnea • Distortion of the normal anatomic appearance • Pain on palpation or with coughing or swallowing • Pain with tongue movement implies injury to the epiglottis, hyoid bone, or laryngeal cartilage • Crepitus (This hallmark sign of disruption to aerodigestive tract is noteworthy in only one third of cases.)
Penetrating the heart, aorta, and great vessels • Hemorrhage, usually associated with large wounds • Massive hemothorax • Hypotension • Tamponade (if intrapericardial portion of aorta is injured) • Weak or absent carotid or brachial pulse • Bruit • Paradoxical pulse (decrease in systolic blood pressure with inspiration) • Cervical or supraclavicular hematoma • Bleeding from the entrance wound • Upper extremity ischemia • Coma • Hemiparesis • Respiratory distress secondary to tracheal compression
Tracheobronchial or lung • Subcutaneous emphysema • Cough • Respiratory distress • Hemoptysis • Tension pneumothorax • Continuous air leak persisting after chest tube insertion • Intercostal retractions • Decreased breath sounds • Agitation • Hypotension • Tachycardia • Hypoxia
Carotid artery • Decreased level of consciousness • Contralateral hemiparesis • Hemorrhage • Hematoma • Dyspnea secondary to compression of the trachea • Thrill • Bruit • Pulse deficit
Jugular vein • Hematoma • External hemorrhage • Hypotension
Esophagus and pharynx • Dysphagia • Bloody saliva • Sucking neck wound • Bloody nasogastric aspirate • Pain and tenderness in the neck • Resistance of neck with passive motion testing • Crepitus • Bleeding from the mouth or nasogastric tube
BIBLIOGRAPHY • http://emedicine.medscape.com/article/827223-overview • Author • David B Levy, DO, FACEP, FAAEM Chairman, Department of Emergency Medicine, St Elizabeth Health Center; Associate Professor of Emergency Medicine, Northeastern Ohio Universities College of Medicine coauthor(s) • Brian S Gruber, MD Clinical Assistant Professor of Surgery, Northeastern Ohio Universities College of Medicine; Clinical Assistant Professor of General/Trauma Surgery, Ohio University College of Osteopathic Medicine; Director, Department of Trauma and Critical Care Services, St Elizabeth Health Center Specialty Editor Board • Edmond A Hooker II, MD, DrPH, FAAEM Assistant Professor, Department of Emergency Medicine, University of Cincinnati College of Medicine; Associate Professor, Department of Health Services Administration, Xavier University Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference Disclosure: Medscape Salary Employment • Eric L Legome, MD Chief, Department of Emergency Medicine, Kings County Hospital Center; Associate Professor, Department of Emergency Medicine, New York Medical College John D Halamka, MD, MS Associate Professor of Medicine, Harvard Medical School, Beth Israel Deaconess Medical Center; Chief Information Officer, CareGroup Healthcare System and Harvard Medical School; Attending Physician, Division of Emergency Medicine, Beth Israel Deaconess Medical Center Chief Editor • Rick Kulkarni, MD Attending Physician, Department of Emergency Medicine, Cambridge Health Alliance, Division of Emergency Medicine, Harvard Medical School