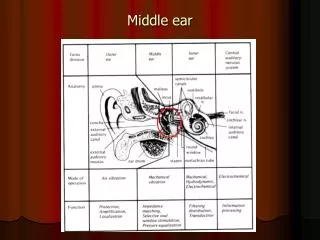
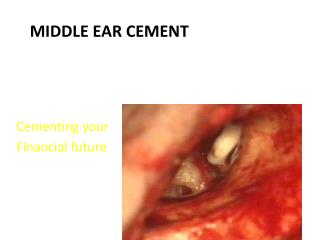
Middle Ear Cement
Cementing your Financial future. Middle Ear Cement. History of SerenoCem in England . Corinthian Medical started in August 1997 License from Sheffield University Cement Corinthian was restructured in April 2003 Renamed Corinthian Surgical. SerenocemTM Cement.

Middle Ear Cement
E N D
Presentation Transcript
Cementing your Financial future Middle Ear Cement
History of SerenoCem in England • Corinthian Medical started in August 1997 • License from Sheffield University • Cement • Corinthian was restructured in April 2003 • Renamed Corinthian Surgical
SerenocemTM Cement • SerenoCem Cement is a bone replacement material • It is classified as an Ionomeric Cement • Ionomeric cements were first developed by Wilson and Kent(1972) for use in dental surgery • 1989 : role in orthopaedic surgery • 1994 :some cases of toxic encephalopathy • 1998 :Biocem on the market • 2000 :SerenocemTM™
Characteristics • SerenocemTM sets by a NEUTRALISATION reaction as opposed to a Polymerisation reaction. • So it is non exothermic • It chemically bonds to: -Bone -Metal (Implant to Implant) - OtomiMix cannot make this claim -itself
Characteristics • Bioactive and Osteoconductive • Minimal Shrinkage • High compressive strength • Biocompatible- the set cement is rapidly surrounded by a layer of bone
Indications • Reconstruction of the Ossicular chain where the cement can be used to repair the bony ossicles in their normal position (BRIDGE THE GAP) • Reconstruction of the outer ear canal • Fixation of cochlear implant array into the Cochleostomy • Fixation of hearing devices – Symphonix Device • Revision of stapedectomy and to secure the loop of the stapes over the incus
Ossiculoplasty Variability • Results of Ossicular reconstruction with implants remain variable • STABLITY of the implants are the #1 concern by all, for styles and suppliers • Recurrent Chronic Otitis media is often unfavourable to both the anatomic and functional success of the surgery • Use of the cement stability can minimize this sequela
Ossiculoplasty Success • Influencing Factors • Quality of the residual Chain • Type and extent of the mucosal disease • Outer ear canal erosion • Shallow tympanic cavity
Ossiculoplasty • Causes of failure • Extrusion - biocompatibility – Tympanoplasty failure • Dislocation : unstable interface between the elements of the repaired chain • Reabsorption : auto grafts /allograft
Ossiculoplasty – Incus gap Remodelled Incus SerenocemTM Crus anterior stapes
Ossiculoplasty SerenoCem Crus posterior stapes Round Window
Canal Wall reconstruction • The posterior canal wall of the external ear canal can be temporarily removed. • This performed in a canal wall up Mastoidectomy by placing two Sharp cuts in the wall one anterosuperior the other posteroinferior once the wall is removed the surgeon performs the surgical steps in a wide open field • The wall is precisely repositioned and fixed with two drops of the cement on the posterior aspect of each cut • SerenoCem is facing the mastoid cavity therefore bone pate is not strictly required except when a musculoperiostal flap is used to fill the bowl
Canal Wall reconstruction • The wall is precisely repositioned and fixed with two drops of the cement on the posterior aspect of each cut • SerenoCem is facing the mastoid cavity therefore bone pate is not strictly required except when a musculoperiostal flap is used to fill the bowl
Fixation of Cochlear Implants • Fixation of the electrode is necessary to avoid slippage of the electrode and avoid displacement because of growth of the mastoid • The cement is put with the bony channel drilled in the temporal bone and the electrode is fixed • ENSURE NO DURAL TISSUE IS EXPOSED
Fixation of Hearing Devices • SerenoCem can be used for the fixation of the Symphonix Implantable Hearing System • It can also be used to strengthen the incus
Revision of Stapedectomy • Where there is an erosion of the long process of the incus causing slippage of the prosthesis • The prosthesis are removed and incudal process is dried the missing segment is remodelled with SerenoCem • SerenoCem can also be used to fixate the pistons instead of crimping
How to use • When the surgeon is ready to use the cement push the coloured piston on the capsule • Place the capsule on the mixer for 10 seconds • Place the capsule into the applicator • Express the cement onto a glass plate by squeezing the handle • CD’s are available................
Placement • Cement must be placed in a dry field • After being activated the surgeon has approximately 3 – 4 minutes working time • Place directly onto bone • Avoid contact with blood or soft tissue until completely set • Once placed the operation site must be kept dry for 10 minutes to allow the cement to set. Setting time can vary depending on temperature • SerenoCem is moisture sensitive prior to setting
SerenoCem Clinicals • Otologic Use of Ionomer Cement Revisited, Babighian G., MD, Department of Otosurgery Azienda Ospedaliera-universita, Padova, Italy • Incudostapedial Rebridging Ossiculoplasty with Bone Cement, Ozer Enver, Otology & Neurotology 2002, 23(5): 643-646 • How we do it: Ionomeric cement to attach the stapes prostheses to the long process of the incus, Tysome, J.R., Clinical Otolaryngology, 30, 458 - 460 You have these
SerenoCem Clinicals • Technical refinements and precautions during Ionomeric cement reconstruction of incus erosion during revision Stapedotomy, Chen, DA and Arriaga, MA, Laryngoscope, 113,5:848-852 • In vivo assessment of CorinCem(SerenoCem) granules by comparison with porous hydroxapatite – a quantitative study • The use of Ionomeric cement in the fixation of cochlear implant, Van de Heyning P, 2001, presented at Int Antwerp Symposium on ME Reconstruction available
SerenoCem HANDS ON
SerenocemTM Handling Trial & Error Instructions Mixer set up • Remove 2 travel screws in base of mixer with Allen Wrenches. • Two red hold down screws Applicator Mixer
SerenocemTM Handling Trial & Error Instructions Mixer the cement • Mixing is done by circulator nurse – non sterile • Two UNSTERILIE practice capsules are provided • Do not sterilize the mixer or applicator • Do not mix until surgeon calls for cement • Surgeon has 3- 4 min after mixed to set up Applicator Mixer
SerenocemTM Handling Trial & Error Instructions To Mix • Press the start button “S” • The Mixer will run 10 seconds and shut off automatically. • Remove the capsule from the mixer • Remove the white clip from the capsule and place capsule into applicator gun Applicator Gun Mixer
SerenocemTM Handling Trial & Error Instructions To Prepare for use 8. Express the entire amount upon the sterile field. • A sterile microscope glass slide works well • Cement is ready to be placed with Rosen Type or Barbara Needle. • Smaller the better
SerenocemTM Handling Trail & Error Instructions Using the Cement • Cement is neurotoxic – when wet. • Cover facial aberrant facial nerve, if present, with neuro-patti or silicone sheeting. • Must be placed into a dry field & will not bond to soft tissue • Let dry 12-15 minutes before closing
Contraindications/warnings • Must not be placed in contact with peripheral nerves, cranial nerves, neural tissue, Dura. C.S.F. or other parts of the central nervous system prior to setting. • Not indicated for acoustic neuroma or skull based surgery • Cannot be used in weight bearing applications • Cannot be used in soft tissue
SerenoCem User Registry • Steve Tilian MD University of Michigan • Alex Arts MD University of Michigan • El-Kashlan Hussan MD University of Michigan • Steve Harvey MD Milwaukee, Wis • Steve Millen MD Milwaukee, Wis • Wesley Kruger MD San Antonio, Tx • Edwin Monsell MD Wayne State, Detroit • Carol Wagart MD North Carolina
SerenoCem User Registry • Perry Phillips MD Sheboygan, Wis. • John Revelis MD Sheboygan, Wis. • James Kemper MD Austin, Tx • Patrick Slatter MD Austin, Tx • Robert Jyung MD University Med/Dental of NJ • Scott Landon MD Baltimore, MD • Loren Bartells MD Tampa, FL • Oleg Fromymovich Minneapolis, MN • Michael Paparella Minneapolis, Mn • Charles Manghan Seattle, Wa • Michael Wong, Seattle, Wa
Conclusion • SerenoCem meets the hot clinical need in today’s Otologic reconstruction surgery: • added Stability • SerenoCem can improve surgery , save time, and give the surgeon the ability to do techniques that were previously not possible. requirements as the cement in the setting
SerenoCem Granules • Granules are a derivative of the cement • Solid porous bone substitute • Due to the solid format the granules do not have the same requirements as the cement in the setting period • They are used for obliteration of the mastoid cavity
Granules • Promotes normal tissue growth • Nonresorbable • Encourage Osteointergration • Easy to use
Application • Mix the granules with blood and a drop of antibiotic until they reach a workable consistency • Place in the cavity • Use minimum amount of granules required • Do not pack tightly or overfill the cavity • Rotate a pedicle flap or similar to cover the granules