Download
1 / 43
440 likes | 1.81k Vues
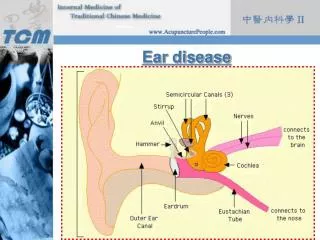
PRESENTATIONS OF MIDDLE EAR DISEASE. Elizabeth Rose Royal Victorian Eye and Ear Hospital Royal Children’s Hospital. A “look and learn” lecture. Middle-ear conditions Management of otitis media Differential diagnosis of ear pain Clinical cases An invitation! (Or Two!).

E N D
PRESENTATIONS OF MIDDLE EAR DISEASE Elizabeth Rose Royal Victorian Eye and Ear Hospital Royal Children’s Hospital
A “look and learn” lecture • Middle-ear conditions • Management of otitis media • Differential diagnosis of ear pain • Clinical cases • An invitation! (Or Two!)
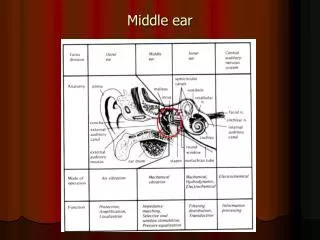
OTITIS MEDIAA SPECTRUM OF DISEASE • acute otitis media • chronic otitis media with effusion • atelectasis of the tympanic membrane • chronic adhesive otitis media • chronic suppurative otitis media • tubotympanic (“safe”) • atticoantral (“unsafe”) and may be acontinuumof disease
ACUTE OTITIS MEDIA(AOM) • the presence of a middle-ear effusion • signs and symptoms of infection • fever, irritability, pain, otorrhoea
Management of AOM • Pain relief Decongestants (oral/topical) and antihistamines • do not make the eustachian tube function better • do relieve the symptoms of a blocked nose
Antibiotic therapy • if severe symptoms - pain - perforation • ≤ 2years of age • immune deficiency • cochlear implant • follow-up not possible
Antibiotic therapy • Recommended treatment is: amoxicillin 50mg/kg/day in 3 doses • Can give up to 100mg/kg/day • Continue for 5 days • If no improvement in 2 days change to amoxicillin/clavulanate
Penicillin allergy • trimethoprim-sulfamethoxazole • clindamycin • ceftriaxone IM, but will often need continuing oral medication
Antibiotic therapy • older children who can be accurate about their symptoms should be treated symptomatically • if no improvement after 2 days consider treatment with antibiotics
CHRONIC OTITIS MEDIA WITH EFFUSION(COME) • the presence of a middle ear effusion • asymptomatic apart from some hearing loss
CHRONIC SUPPURATIVE OTITIS MEDIA(CSOM)“deafness and discharge” • persistent disease • insidious onset • severe destruction • irreversible sequelae
1. tubotympanic disease(“safe”) central perforation 2. atticoantral disease(“unsafe”) cholesteatoma the presence of keratinising squamous epithelium in the middle ear
MANAGEMENT OF CHRONICOTITIS MEDIA WITH EFFUSION(and also retraction/atelectasis of the tympanic membrane)
AKA • grommets • tubes • pressure equalisation tubes • middle ear ventilation tubes
COME Who should have middle ear ventilation tubes?
1. COME for 4 months at least, with hearing loss 2. COME in a child ‘at risk’ regardless of the hearing 3. COME and structural damage to the tympanic membrane
1. Hearing loss • median hearing loss is mild but there is a wide range • no data on the criteria for what is a significant hearing loss
50% of children with persistent OME have hearing thresholds at 20 dB
20% of children with persistent OME have hearing thresholds at >35 dB
2. An ‘at risk’ child has an increased risk of developmental difficulties due to: physical sensory cognitive behavioural factors not related to the OME
‘At risk’ • Suspected or diagnosed speech and language delay or disorder • Autism-spectrum disorder and other pervasive developmental disorders • Blindness or uncorrectable visual impairment
Management of the ‘at risk’ child may include: • speech and language therapy along with management of the OME • hearing aids for hearing loss independent of the OME
Children with persistent OME who: • are not ‘at risk’ • do not have significant hearing loss • donothave structural abnormalities of the eardrum or middle ear should be examined every three months
PAIN (Otalgia)
DIFFERENTIAL DIAGNOSIS OF EAR PAIN A.External auditory canal • trauma ( e.g. from cotton bud abuse) • auricular haematoma • foreign body • otitis externa • external auditory canal tumour
DIFFERENTIAL DIAGNOSIS OF EAR PAIN B. Middle ear • acute otitis media • bullous myringitis • chronic suppurative otitis media • middle ear tumour
DIFFERENTIAL DIAGNOSIS OF EAR PAIN C. Referred pain • oropharynx (IXth nerve) • tonsillitis/post-tonsillectomy • carcinoma, including posterior tongue • laryngopharynx(Xth nerve) • pyriform fossa • upper molar teeth, TMJ, parotid gland(Vc) • impacted wisdom teeth • changes to bite from new dentures • cervical spine(C2, C3) • pain is often worse at night
DISCHARGE (Otorrhoea)
YOUARE INVITED! 1. ENT clinics at RVEEH
All clinical years students Every week day afternoon (and some mornings)
ContactRehana De Jong 9929 8666 RehanaDeJong@eyeandear.org.au
YOUARE INVITED! 2. Hedley Summons Otolaryngology Prize
All clinical years students from University of Melbourne Coming in September!
Take-home message 2more is missed in medicine by not looking than by not knowing
ENT clinic Fifth Floor Outpatients 9929 8666 RehanaDeJong@eyeandear.org.au