The Air We Breath
By: Diana Blum MSN Metropolitan Community College. The Air We Breath. Objectives. Describe the normal anatomy and physiology of the respiratory system. Discuss the data to be collected from the client with a respiratory disorder.

The Air We Breath
E N D
Presentation Transcript
By: Diana Blum MSN Metropolitan Community College The Air We Breath
Objectives • Describe the normal anatomy and physiology of the respiratory system. • Discuss the data to be collected from the client with a respiratory disorder. • Describe the nursing implications of age-related changes in the respiratory system. • Describe selected diagnostic tests and procedures for respiratory disorders and identify the related nursing interventions. • Describe the basic pathophysiological changes, symptoms, data commonly collected, diagnostic medical treatment, and nursing interventions for the following conditions: Acute viral rhinitis, influenza, pleurisy, pneumonia, pneumothorax, pulmonary embolus, acute respiratory distress syndrome. • Recall from pharmacology the selected drug classifications used to treat diseases of the respiratory system and list nursing interventions associated with each. • Discuss the basic pathophysiology, risk factors, symptoms, data commonly collected, diagnostic tests, medical treatment, and nursing interventions for chronic obstructive pulmonary disease to include: Asthma, chronic bronchitis, and emphysema. • Discuss the basic pathophysiology, risk factors, symptoms, data commonly collected, diagnostic tests, medical treatment, and nursing interventions for restrictive pulmonary disease to include: Tuberculosis and lung cancer. • Describe nursing assessments and interventions utilized when caring for a client following thoracic surgery. • Discuss the nursing process as it relates to the respiratory system. • Discuss nutritional concepts as they relate to the care of a client with a respiratory disorder.
Respiratory System • Focuses on the energy required to carry out ADL. When lung tissue is damage and 02 at cellular level is severely decreased the client may not be able to perform any of these functions. Energy conservation tech are most important!
Nursing Diagnosis • Pain r/t inflammation, tissue damage • Ineffective breathing pattern r/t surgical incision, pleural effusion, decreased lung expansion • Impaired gas exchange r/t alveolar destruction, bronchospasm, air trapping • Ineffective airway clearance r/t weak cough • Anxiety r/t hypoxemia • Activity intolerance r/t inability to meet 02 needs • Decreased cardiac output r/t pump failure (r-sided) • Imbalance nutrition: less than body require r/t anorexia, dyspnea
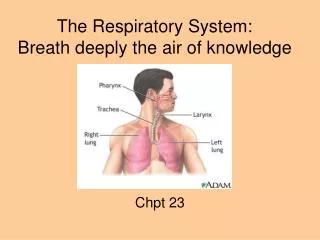
Pathways • Nose to pharynx}behind the mouth to esophagus (approx. 5 inches) • Larynx} voice box: air passes between pharynx and trachea • Trachea} windpipe • Bronchi}this is the main branch that air passes through divides into left and right branch • Bronchioles} subdivides and connects with alveoli for gas exchange
More anatomy • Epiglottis} behind the thyroid cartilage • Has a hinged door action to larynx • Glottis} space between the folds of vocal cords • Air from the lungs promote it to open and close • Lungs} 3 lobes on the right and 2 lobes on the left • Pleura}membrane that covers the lungs • Has a lubricant between the layers to allow inhalation and exhalation to occur • Cilia} hair like projections that trap debris
Fun facts • Mucous membranes warms and moistens the air that passes to and from the lungs • Upper respiratory tract consists of: the outside chest, nose, mouth, pharynx, larynx • Lower respiratory tract consists of: inside the chest, trachea, bronchi, bronchioles, alveoli
Mechanism of breathing • Inspiration : air enters lungs • Active process where Chest muscles and diaphragm contract causing chest cavity to enlarge • Expiration: air leaves lungs • Passive process where muscles relax and the chest returns to normal. • Normal quiet breathing = 500ml of air exchanged with each breath
Apnea • Temporary interruption in the normal breathing pattern in which NO air movement occurs • May occur during sleep and at end of life • http://abcnews.go.com/Video/playerIndex?id=2927688
~pnea • Dyspnea} difficulty breathing or shortness of breath • Orthopnea} difficulty with breathing while in a lying position • Tachypnea} respiratory rate >20 • Bradypnea} respiratory rate <12 • Other breathing types located in table 30-1
Data Collection • Past history/Family history: colds, TB, Chronic bronchitis, asthma, cancer, sinus infections, ear infections, pneumonia, COPD, emphysema, allergies, immunizations, diabetes, CAD, TB tine, Smoking history (pack per year history) • Chief complaint: obtain details on subjective complaints r/t respiratory system • Cough: onset, duration, severity, frequency (consistency, odor, amount, color), type (wet/dry), sputum production • Dyspnea: onset, duration, severity, precipitating events, associated symptoms like fatigue or palpitations • Pain: (chest) : location, onset, duration, precipitating events (trauma, coughing, inspiration), radiation, associated symptoms like fever, sweating, nausea • Look at what meds were taken to attempt relief
Examination • Ask for subjective info about fatigue, weakness, fever, chills, nasal obstruction, sinus pain, hoarseness, edema, sore throats • Functional assess: occupation, exposure to pathogens, respiratory irritants, usual diet, role in family, stressors, coping strategies • General: appearance , facial expression, posture, alertness, speech pattern, observable distress, VS, Ht, Wt, nasal shape, nasal tenderness, flaring, swelling, discharge, bleeding, septal deviation, sinus tenderness, pursed lip breathing, lip color, throat color, tonsil appearance, trachial alignment, enlarged lymph nodes , lung sounds, breathing pattern, use of accessory muscles, abd distention, color of extremities, clubbing, homan’s sign, edema, cyanosis.
Lung sounds • Normal Breath Sounds • To be able to distinguish between types of abnormal breath sounds and their location, it is important to understand normal respiration and its effect on airway noises that make up breath sounds. Normal breath sounds are bronchovesicular in nature. They are loud pipe-like sounds in the large airways, and softer blowing-like sounds in the small airways. Normal breath sounds are loudest during inspiration and softest during expiration. The inspiratory phase is shorter with faster airflow. Although abnormal sounds may be louder during inspiration, they may be difficult to distinguish due to their short duration. • Normal Air Flow through the Lungs • Flow is greatest in the trachea and diminishes in the distal lung fields, until it reaches the alveoli, where there is no flow. Breath sounds are loudest over areas with greater flow, and distal pathology may be communicated to these areas. Therefore, auscultation over the trachea may reveal pathology there or communicated from distal regions of the lung. • **If breath sounds are really diminished, listen over the trachea** • Adventitious sounds • Wheezing: musical, whistling sound • Usually more pronounced during expiration • From narrowed airways • Bronchoconstriction • Secretions • Interventions: • Bronchodilation • Hydration • Coughing • http://www.ed4nurses.com/breathsnds.htm • Rales: crackling sound • Heard at the end of inspiration • From collapsed or waterlogged alveoli • Fine: beginning of fluid buildup / or atelectasis • Coarse: greater volume of fluid buildup • Interventions: • Manage fluids • Budget volume resuscitation • Diuretics • Expectorate • Turn & position • Deep breathing • Forced expiration • Vibration & percussion • Rhonchi: bubbling • The sound will be heard throughout inspiration and expiration. • Louder than rales due to larger secretions • Results from air bubbling past secretions in the airways • Interventions: • Deep breathing • Coughing • Hydration (encourage fluids, if no restriction) • Humidify air • Mobilize • Friction rub: creaking, leathery sound • End of inspiration and beginning of expiration • Caused by rubbing of inflamed pleural surfaces against lung tissue. • Interventions: • Chest x-ray • Anti-inflammatory medications
Lungs sounds continued Cheyenne Stokes Kussmal’s • Breaths are deep than become shallow followed by periods of apnea • Cause: severe brain pathology • Regular breathing but breaths are deep • Rates are >20 bpm • Causes: metabolic acidosis, renal failure, diabetic ketoacidosis
http://rnbob.tripod.com/breath.htm • Lung sounds http://www.med.ucla.edu/wilkes/lungintro.htm • http://www.rnceus.com/resp/respabn.html • case studies http://www.meddean.luc.edu/lumen/MedEd/medicine/pulmonar/pd/step29e.htm
Age related changes • Muscle atrophy in pharynx and larynx and change in vocal cords • Loss of lung elasticity • Decreased number of alveoli • Weaker chest muscles • Diminished chest movement • Less effective cough • Work harder to breath • Enlargement of bronchioles • More suseptible to lung infections r/t decreased defense mechanisms • Rib cage becomes more rigid and diaphragm flattens
Diagnostics • Chest xray • Fluoroscopy: observes deep structures in motion, can look at both lungs at same time • Looks at speed and degree of lung expansion and looks for structural defects • No jewelry on neck or chest, no clothes from waist up except hospital gown • Ventilation/Perfusion Scan: used to detect pulmonary embolisms, or other obstructions • IV or inhaled radioactive med given • NPO for 4 hours prior to. • Monitor for anaphylaxis • Radioactive material is excreted in urine • Inform importance of hand washing and if anyone else handles urine they should glove as well
Diagnostics continued • Cat scan: visualize lesions • Needs to be still • With or without contrast • Check for iodine allergy • IV access • MRI: looks for tumors, lesions, etc. • Lie flat, mechanical noises • NO metal allowed • Pulse oximetry: non invasive method to evaluate o2 levels in blood • May be continuous or intermittent • Small censor on finger or ear • Indicate level of oxygen with result
Diagnostics continued • PFTs: used to diagnose disease, monitor progression, assesses medications • Measures lung volumes and capacities • Total lung capacity, forced expiratory volume, functional residual capacity, inspiratory capacity, vital capacity, forced vital capacity, minute volume, and thoracic gas volume (table 30-2) • A clip is placed on the nose that the patient breathes through a mouth piece to determine mechanics (flow rates of gas in and out of lungs) and diffusion (movement of gas across aveoli/capillary membrane) • ABGs: measures the concentrations of oxygen and carbon dioxide in the arterial blood to determine if exchange is adequate across the alveolar membrane • pH: 7.35-7.45 • PaCo2: 35-45 • PaO2: 80-100 • HCO3: 22-26 • Sats: 96-100 • http://www.youtube.com/watch?v=IBJtQtzN7O8&feature=related • http://www.youtube.com/watch?v=Xsr5wF-WDrw&feature=related • http://www.youtube.com/watch?v=7s6OGhMfUqI&feature=related • http://www.youtube.com/watch?v=LcmjGMWDbXw&feature=related • http://www.youtube.com/watch?v=t9x4tB9GOi8&feature=related
Diagnostics Continued • Bronchoscopy: performed by inserting a small camera through the nose or mouth into the bronchial tree under local anesthesia • It allows direct visualization of structures • Explain procedure and assess allergies • Consent needs to be obtained • NPO 6-8 hours prior • No smoking days prior • dentures removed and document loose teeth • Administer sedatives as prescribed (cetacaine) • Atropine may also be given to decrease secretions • post procedure: • NPO until gag reflex returns • Semi fowler’s position • Monitor vitals • Monitor for edema, hemoptysis, stridor, asymmetric movement of chest • Report abnormal findings to doctor! http://www.youtube.com/watch?v=DS6MHZCGlJk
thoracentesis • Removal of pleural fluid for examination or to allow for lung re-expansion • Obtain consent • Post : • Assess respiratory status • Document amount, color of fluid • Monitor dressing for bleeding • Label specimen bottle and send to lab http://www.youtube.com/watch?v=noDxydboLrA&feature=related
Diagnostics continued • Tuberculin test (A.K.A. TB Tine) • Determines past or present exposure to tuberculosis • Pre: • Inform the client about intradermal need stick • Cleanse skin and inject intradermally into lower anterior forearm • Mark and record site • Instruct pt that skin reaction can last 1 week and not to scratch it. • Inform patient they need to return in 48-72 hours for interpretation of positive or negative response • ***Reddness, swelling of 5mm or more is considered positive • A pt with a history of BCG vaccination (foreign born) will always test positive regardless of exposure. • Post: follow up depends on response. • If positive pt will be sent for chest x-ray to confirm active tuberculosis
Diagnostics Continued • Sputum analysis} the mucous membrane lining in the lower respiratory tract responds to acute inflammation by producing an increase in secretions • Specimens are examined for volume, consistency, color, odor • Sputum that is thick, foul smelling, and yellow, green, or rust colored may indicate bacterial infection • Pt needs to expectorate the specimen into a sterile container after coughing deeply if unable induction may need to be done to obtain • C & S} determines presence of bacteria, id’s specific organism, and appropriate treatment • Acid fast} done to determine the presence of acid fast bacilli including TB. Collection is 3 samples • Cytologic} used to determine the presence of carcinoma or infection. Special collection chamber is needed. Ask facility laboratory. • CBC: • Hemoglobin-assess 02 carrying capacity • WBCs- assess increase r/t infection
Breathing exercises • Cough and deep breath (pg. 522) • Incentive Spirometry: instruct the pt to use 10 times every hour awake or with every commercial break if watching t.v. • Purse lip breathing: pucker lips like you are going to blow a kiss, whistle, or blow out a candle. Inhale through the nose and exhale through the pursed lips. Exhalation should last longer than inhalation. • Percussion and vibration • Percussion} clapping of cupped palms against chest wall to dislodge secretions ( only in areas protected by the rib cage) lasts 20-30 secs • Vibration} as pt exhales the therapist creates a shaking movement with the palms • Contraindications for both include: lung ca, bronchospasm, hemorrhage, hemoptysis, increased ICP, chest trauma, PE, pulmonary edema, GERD, anxiety, rib fractures http://www.youtube.com/watch?v=8rI5y2hyC2c&feature=related • Postural Drainage ( page 523-524)
Suctioning • Goal} improve to improve oxygen and CO2 exchange by removing excess mucus with a suction catheter…Follow facility guidelines! • Procedure: • Use sterile technique for tracheal and clean technique for oral. • Administer O2 before inserting catheter WHY? • Moisten cath in sterile water and insert through nose or mouth before applying suction • Apply suction as the catheter is withdrawn from the airway • Maintain pressure gauge b/w 80-100 mmHg • Limit EACH pass to 10 seconds • Allow the patient to rest briefly, encourage deep breathing and rinse catheter with sterile water before each pass. • Monitor for patient’s response • If tachycardia or increased respiratory distress develops, stop the procedure immediately and give the patient oxygen as ordered • Document the amount, color, odor, and consistency of the secretions as well as pt status before and after procedure.
Nasal Cannula: 1-6 liter flow Simple mask: 6-10 liters/FiO2 35-55% Partial rebreather: has reservoir bag so patient can rebreath part of inhaled gas: 6-10 liters/ FiO2 35-60% Non rebreather: non of exhaled gas rebreathed. FiO2 70-100% (venturi mask)
Monitor O2 • Monitor liter flow to make sure it is as prescribed. Assess pt response to therapy (ABGs as ordered) • Maintain sterile water in the humidity reservoir • Clean and replace equipment according to agency policy • NO SMOKING signs need to be posted if not a smoke free facility
Artificial Airways • Oral: temporary tube that rests at base of tongue • Nasal: (trumpet) soft rubber tube inserted through nose to tongue. Rotate nares q8 hours • Endotracheal: these have cuffs. From mouth or nose to trachea. Prevents aspirations and facilitates mechanical ventilation. • Tracheostomy: surgical airway created through neck. May or may not have cuffs • See mechanical vent handout
Care after thoracic surgery • Manage pain with attention to resp status HOB elevated!! • VS as per post-op protocol & relate to client’s norms • Assess resp closely: rate, rhythm, effort • Lung sounds, chest rising and falling with each resp • Note absence of cyanosis or dyspnea • Maintain patent airway, TCDB, IS q 1 hour while wake, suction prn • Care to chest tube and drainage system • 02 responsibilities based on ABGs-02sats • IV responsibilities • Provide for a safe environment r/t: pain meds • Wound assessment and care as ordered • Activity progression as ordered and tolerated • I&0 q 8 hours to include chest tube • Assess lab: h&h, lytes, bun and cr, PT/INR, PTT, CBC
Chest Tubes • Chest tubes are inserted to drain blood, fluid, or air and allow full expansion of the lungs. The tube is placed in the pleural space. The area where the tube will be inserted is numbed (local anesthesia). The patient may also be sedated. The chest tube is inserted between the ribs into the chest and is connected to a bottle or canister that contains sterile water. Suction is attached to the system to encourage drainage. A stitch (suture) and adhesive tape is used to keep the tube in place. • The chest tube usually remains in place until the X-rays show that all the blood, fluid, or air has drained from the chest and the lung has fully re-expanded. When the chest tube is no longer needed, it can be easily removed, usually without the need for medications to sedate or numb the patient. Medications may be used to prevent or treat infection (antibiotics). http://www.atriummed.com/PDF/ManagingChestDrainage.ppt#438,37,Remove fluid & air
Tidaling: the middle water seal chamber is observed for expected rise in fluid level with expiration. • Air leak: noted when continuous bubbling is observed in the main water seal chamber • Suction may be wet or dry • A gentle bubbling sound is normal to hear with a wet system • Dry systems have a orange accordion looking object visible when suction is applied • Change the recepticle only when chambers are full using sterile technique • Heimlich Flutter Valve: air and fluid are expelled and not rebreathed in • READ THORACIC SURGERY page 530-531
Drug Therapy • Corticosteroids: Used to decrease inflammation and edema • May be given parenteral, oral, inhaler • Many SE, masks S/S of infection, cause F&E imbalances • NI: Rinse mouth after each inhaler use, instruct to not to d/c abruptly, takes up to 10 days to obtain a blood level • Decongestants: mimics epinephrine, (stimulates HR and BP increases) cause vasoconstriction, reduces mm swelling—example: sudafed • NI: monitor pulse, BP, mental status • Avoid if HTN, DM or hyperthyroid clients
Drug Therapy Continued • Bronchodilators: Relax smooth muscles in the bronchial tree & help widen the passageway • Used for asthma and COPD • May be given oral, IV, by Inhalation • Does stimulate CNS and cardiac activity • Aminophyline, Isuprel, Brethine, Atrovent, Albuterol NI: Monitor HR, oral hygiene, avoid caffeine • Antitussives: Decreases frequency and intensity of cough by suppressing cough reflex but without eliminating it • Codeine popular but is a narcotic • Dextromethorphan is non-narcotic • NI: force fluids
Drug Therapy Continued • Antimicrobials: Will kill or inhibit the growth of bacteria, virus, or fungi • Obtain C & S before administration of 1st dose • NI: Assess for allergies • Instruct on importance of taking all of prescription • Mast Cell Stabilizers: Helps prevent asthma attacks by preventing the release of histamine and slow-reacting substance anaphylaxis (SRS-A) • Does not help after onset of S/S • Intal (cromolyn) most common med • NI: instruct to use prior to activity • Expectorants: Given to thin secretions • Pill or syrup form • Robitussin is a popular OTC • NI: assess effectiveness of cough
Drug therapy Continued • Antihistamines: Block allergic responses. (Histamine 1 blockers) • Can be purchased without prescription • Dry MM • Mild sedation and antiemetic effects • Benadryl (1st generation) • Claritin (2nd generation) • May worsen cough by drying bronchial secretions • Not recommended for clients with asthma • NI: Care with operating machinery, being in a situation where sound judgment is imperative. Avoid alcohol
Acute Viral Rhinitis • common cold—lasts 2-14 days • Inflammation and edema of nasal mm • Based on H&P • S/S: nasal stuffiness, sneezing, running nose, ha, sore throat, fatigue, fever • Most contagious first 3 days • NI: Prevent spread of infection-handwashing, proper disposal of tissue • Rest, fluids to exceed 3000ml • Humidifier, antipyretics, analgesics • Call MD if T > 101, severe sore throat with white patches, chest pain, purulent sputum
Influenza • Several strains and more common in winter • Is an acute viral respiratory infection with fever and aches, chills, ha, cough • Complications: bronchitis, pneumonia • Spread by droplet/physical contact • Incubation 1-3 days, illness lasts 2-8day • NI: Rest, fluids, balanced diet, antipyretics, analgesics, antiviral agents (which must be started 24-48 hours after S/S) • Use of immunizations to prevents – 70-90% effective • Go to MD office only if chest pain or increase on chest congestion.
Pneumonia • Bacteria often pneumococcus which releases toxins=inflammation=damage • Viral, fungal, hypostatic, aspiration, nosocomial, chemical • Classified by location: lobar, bronchial • At risk: smokers, altered LOC, immunosuppressed, chronically ill, tube feeders, trach and ET tube clients
Pneumonia Diagnosis • H&P • C&S of sputum • CXR • WBC • Blood cultures
S/S • Chills, fever, sweats, chest pain, cough, purulent sputum production, hemoptysis, dyspnea, headache, herpes simplex, leukocytosis (WBC=20,000-30,000), tachycardia, crackles, wheezes, N/V • ****Elderly=confusion • Complications: Pleurisy, Pleural-effusion
NI • HOB > 30-45 degrees, keep warm and dry, VS q 4 h, assess lung sounds, skin color and signs of hypoxia • What Is Hypoxia? • FF, I&O q 8 h, freq oral cares, care of expectorations, safety precautions r/t fever, fatigue • TCDB q 2h, measures to mobilize secretions, hi protein diet • Assess fluid and electrolyte balance
Pleurisy • Inflammation of the pleura • Causes: pneumonia, TB, injury • S/S abrupt / severe pain. Breathing and coughing aggravates • Tx: analgesics, anti-inflammatory, antitussives, antimicrobials, heat • NI: Assess and Tx pain, Splint with cough, HOB >, meds as appropriate
Chest trauma • 2 types: penetrating and non penetrating • Penetrating: stab wounds , gun shot wounds • Non penetrating: MVA, Falls, blunt injuries • S/S: visible trauma, chest pain, Dyspnea, cough, asymmetric movement, cyanosis, rapid weak pulse decreased blood pressure, tracheal deviation, JVD, bloodshot or bulging eyes • Tx: stablize and prevent further injury, remove clothing to assess injury and observe for other injuries like bleeding. Immediately treat the bleeding cover chest wound and tape on 3 sides
Pneumothorax • Accumulation of air in the pleural cavity resulting in complete or partial collapse of the lung. • Spontaneous (smokers, blebs) • Tension pneumothorax-air entering space > causing pressure on heart and great vessels • Diagnosis: CXR, H&P • S/S:dyspnea, tachypnea, tachycardia, restlessness, pain, anxiety, decreased movement in chest wall, < lung sounds, progressive cyanosis, sucking chest wound with open pneumothorax. • TX: Chest tube insertion to remove air or fluid • Closure of open chest wound or tear in structures • NI: Fowlers or semi-Fowlers http://video.google.com/videoplay?docid=1169503917162980359&q=%22chest+tube+%22&total=14&start=0&num=10&so=0&type=search&plindex=1