Download
1 / 34
380 likes | 901 Vues
Our therapeutic concept Transoral lasermicrosurgical resection if preservation of organ seems feasible Selective neck dissection ( N0 – N2 ) Postoperative radio (- chemo) therapy for advanced neck disease. Cancer of the Larynx and Pharynx. Cancer of the Larynx and Pharynx.

E N D
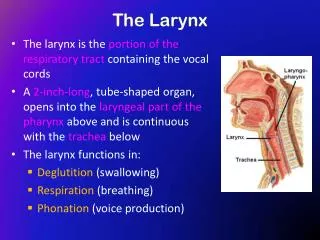
Our therapeutic concept Transoral lasermicrosurgical resection if preservation of organ seems feasible Selective neck dissection ( N0 – N2 ) Postoperative radio (- chemo) therapy for advanced neck disease Cancer of the Larynx and Pharynx
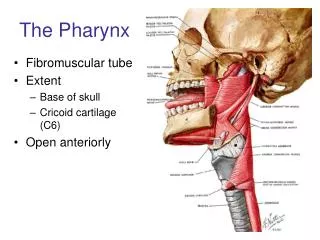
Cancer of the Larynx and Pharynx The main principle is to minimize the surgical morbidity while not compromising time honored oncological principles
Cancer of the Larynx and Pharynx Prerequisites • Experience of the surgeon • Adequate exposure • Careful histological examination • Cooperation of the patient acceptance of possible re-resection, follow up and the abandoning of carcinogenic habits
Cancer of the Larynx and Pharynx Preconditions for organ preservation • Larynx:preservation of at least one arytenoid cartilage • Hypopharynx:preservation of half of the larynx circumference of hypopharynx about 2 cm No extensive spread to the neck
Cancer of the Glottis pT2/pT3 n=338 Therapy pT2apT2bpT3 n=128 n=115n=95 Laser 116 (91%) 87 (76%) 42 (44%) Laser + ND 12 15 41 Laser + RAD - 11 3 Laser + ND + RAD - 2 9 University of Göttingen, Germany 05/2005
Cancer of the Glottis pT2/pT3 n=338 Postoperative Complications ( n= 10 / 3 % ) pT2a pT2bpT3 n=128n=115n=95 Postop. Bleeding (MLS) 1 1 1 Glottic stenosis (MLS) 0 0 1 Laryngeal edema (MLS) 0 0 2 Tracheotomy 0 0 3 Pneumonia 1 0 0 Department of Otorhinolaryngology, Head and Neck Surgery University of Goettingen, Germany 04/2005
Cancer of the Glottis pT2/pT3 n=338 Recurrence-free Survival 82,1% pT2a 61,4% pT2b Recurrence-free survival [%] pT3 60 % Time [months] University of Göttingen, Germany 05/2005
Cancer of the Glottis pT2/pT3 n=338 Overall Survival 74,5% Overall survival [%] pT2a 64,6% pT2b 57,6% pT3 Time [months] University of Göttingen, Germany 05/2005
Supraglottic Carcinoma n=216 Therapy Stage III Stage IV n=65n=68 Laser 12 - Laser + ND 42 36 Laser + RAD 1 - Laser + ND + RAD 10 32 Universitäts-HNO-Klinik Göttingen 05/2005
Supraglottic carcinoma n=216 Postoperative Complications pT1/pT2 pT3/pT4 n=95n=121 Postop. bleeding (MLS) 5 13 Laryngeal edema (MLS) 1 4 Laryngeal stenosis 1 3 Pneumonia 2 2 Department of Otorhinolaryngology, Head and Neck Surgery University of Goettingen, Germany 04/2005
Supraglottic carcinoma n=216 Tracheotomy pT1/pT2 pT3/pT4 n=95n=121 Prophylactic 1 3 Aspiration 0 2 Edema 1 1 Stenosis 0 2 Postop. bleeding 0 1 Department of Otorhinolaryngology, Head and Neck Surgery University of Goettingen, Germany 04/2005
pT3 and pT4 Supraglottic Carcinoma (n=121) pT3 pT4 (n=76) (n=45) 5y local control rate [%] 79 69 Salvage laryngectomy [%] 5 16 5y overall survival rate [%] 67 54 5y rec.-free survival rate [%] 67 60 median follow-up interval: 52 months 12/2002
Piriform Sinus Carcinoma (n=129) Stage Distribution (UICC 1992) a
Piriform Sinus Carcinoma (n=129) Postoperative and late complications Postoperative Hemorrhage 5 (3.9%) - endoscopic coagulation 4 - endoscopic coagulation, tracheotomy 1 Postoperative Edema 1 (0.8%) - microlaryngoscopic removal of mucosa Posttherapeutic hypopharyngeal stenosis 1 (0.8%) - gastrostomy tube
Piriform Sinus Carcinoma n=129 Local recurrence Loco-reg. rec. UICC 92 No. % No. % pT1 n=24 2 8.3 0 0 pT2 n=74 5 6.7 3* 4.1 pT3 n=17 2 11.8 0 0 pT4 n=14 3 21.4 2 14.3 * 1 x kontralaterally 04/2000
Piriform Sinus Carcinoma (n=129) Salvage Therapy of Local and Locoregional Recurrences (n=17) No. % Laser microsurgery 5 29 Laser microsurgery + radiotherapy 3 18 Partial pharyngectomy with laryngeal preservation 1 6 Partial pharyngectomy with total laryngectomy 1 6 Palliative treatment 6 35 Unknown 1 6
Piriform Sinus Carcinoma (n=129) Recurrence-free Survival 95% 69% 01/2000
Piriform Sinus Carcinoma (n=129) Overall Survival 71% 47% 01/2000
Advantages are based on the following: • Transoral approach • Use of the operating microscope • Specific cutting properties of the CO2-laser • Transecting tumor tissue
Advantages ( 1 ) • Laser surgery repeatable at any time ( residual, recurrent, 2nd primary ) • All surgical options available during or after laser resection • Integration into any therapeutic concept • Early postoperative radiotherapy possible
Advantages ( 2 ) • Low peri- and postoperative morbidityRarely tracheotomy or feeding gastrostomy No blood transfusion • Low complication rate No fistulas or carotid blow out Rarely significant edema Rarely perichondritis or chondronecrosis
Advantages ( 3 ) • Duration of operation, hospital stay and rehabilitation are shorter • Lower costs • Professional and social reintegration earlier and more effective • Favourable psycho-oncologic effects
Glottic Cancer pT1an=333 (5-year Kaplan-Meier Estimates) • Local Control → 96.2 % • Disease specific surv. → 100 % • Overall Survival → 86.8 % • Larynx Preservation Rate →97.6 % • Complication Rate → 1.2 %
Results AC+ - anterior commissure involvement; AC- - no anterior commissure involvement; LE - salvage total laryngectomy for advanced recurrence.
Transoral Carbon Dioxide Laser Microsurgery for Recurrent Glottic Carcinoma after Radiotherapy Department of Otorhinolaryngology – Head and Neck Surgery University of Göttingen, Germany 34 patients with recurrent glottic carcinomas after radiotherapy were treatedby laser microsurgery between 1987 and 1998 Primary tumor classification before radiotherapy Classification of recurrence after radiotherapy
Organ Preservation and Survival • 24 patients (71%) were cured with one or more (up to 4) laser procedures. • In 9 patients (27%) recurrences could not be controlled by laser microsurgery. 6 (18%) patients underwent total laryngectomy, 3 patients (9%) underwent palliative treatment. • One patient received total laryngectomy because of chondronecrosis after laser treatment. • Overall 3-year (5-year) survival rate was 74% (53%). • The Kaplan-Meier 3-year and 5-year disease-specific survival was 86%.
Conclusion • In early and advanced stage recurrent glottic carcinomas after primary radiotherapy, C02 laser treatment can be recommended for early and advanced glottic carcinomas as a curative organ preserving procedure with favourable functional results.