Foam Rolling, Stretching, Mobility Training
Foam Rolling, Stretching, Mobility Training. Foam Rolling . Is it changing in the fascia? Trigger point release? DNIC? Physiological results vs , physical results . What is it?.

Foam Rolling, Stretching, Mobility Training
E N D
Presentation Transcript
Foam Rolling • Is it changing in the fascia? • Trigger point release? • DNIC? • Physiological results vs, physical results
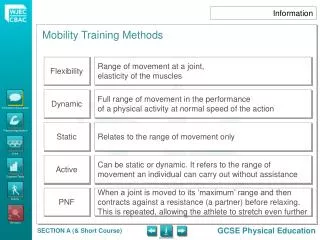
What is it? • Foam rolling is a common form of self- myofascial release that is often used by fitness enthusiasts and athletes prior to a workout with a view to improving flexibility or after a workout with a view to reducing muscle soreness and promoting quicker recovery
Thought to improve muscular function, performance, and joint range of motion
Fascia • fascia is the soft tissue component of the connective tissue system that both penetrates and surrounds muscles, bones, organs, nerves, blood vessels and other structures and extends from head to toe, from front to back, and from surface to deep in an uninterrupted, three-dimensional web. Schleip (2012) also define fascia as “the soft tissue component of the connective tissue system that permeates the human body (and) that is part of a body wide tensional force transmission system.”
A dense fibrous connective tissue that connects muscles, bones, and organs, forming a continuous network of tissue throughout the body.
What does fascia do? • Maintaining structural integrity • Providing support and protection • Acting as a shock absorber • Plays a role in hemodynamic and biochemical processes • Provides the matrix permitting intercellular communication • Functions as the body’s first line of defense against pathogenic agents and infections • Creates an environment for tissue repair post-injury
Fascia Changes? • The temporary nature of the results strongly suggests a nervous system mediated mechanism for efficacy, not a structural one.
Thixotropic property of fascia • This theory explains that when undisturbed fascia becomes more viscous and takes on a more solid form, which can restrict movement. • If heat from rolling friction, mechanical stress, massage, or pressure is applied to the fascia, it can become more gel like and pliable, allowing for a greater ROM
Rolf- “connective tissue is a collodial substance in which the ground substance can be influenced by the application of energy (heat or mechanical pressure) to change its aggregate form from a more dense ‘gel’ state to a more fluid ‘sol’ state
Solid Theory? • Does a poor job of explaining what actually happens • The problems of reversibility arise • In collodial substances the thixotropic effect last only as long as the pressure or heat is applied. Within minutes the substance returns to its normal state
Trigger Points • The technical definition involves several elements such as a hyperirritable nodule within a palpably taut band that elicits a twitching response to snapping palpation. Trigger points are thought to be caused by some sort of metabolic crisis in the muscle cells which causes chemical irritation in the local area and for some unknown reason refer pain to other areas when pressed.
the dominant theory is that a trigger point (TrP) is a small patch of tightly contracted muscle, an isolated spasm affecting just a small patch of muscle tissue (not a whole-muscle spasm like a “charlie horse” or cramp9). That small patch of knotted muscle cuts off its own blood supply, which irritates it even more — a vicious cycle called “metabolic crisis.”
The problem with mechanical models • the research showed quite clearly that the forces required for plastic deformation of fascia significantly exceed what can be applied to it with hands. • In the case of fascia lata, a predicted normal load of 9075N (925kg) and a tangential force of 4515N (460kg) are needed to produce even 1% compression and 1% sheer. Such forces are far beyond the physiological range of manual therapy.
DNIC • Diffuse noxious inhibitory control (DNIC) is one of several varieties of “descending modulation”, by which the brain adjusts the “volume” on nociception (danger signals which originate in the body). DNIC means that the brain inhibits nociceptive signals from traveling up the spinal cord to the brain.
DNIC is a powerful but temporary way to reduce pain in one area by creating pain in another. It depends on a decision by the brain to ignore danger signals from the body. Expectation of benefit from the irritating stimulus plays a strong role
Rule number one in foam rolling is to find a sore spot and stay on it for some time. You need to create some pain. Of course, the pain is often a “good pain”, which is exactly the type of feeling that would correlate with the brain’s conclusion that the irritation is somehow beneficial – which is what gets DNIC going.
You put a foam roller into your butt and create some significant nociceptivesignalling. The brain receives it and says something like: “OK, the butt is telling me that there is some danger down there right now. But I happen to know that this is a therapeutic situation because my trainer said so. So, let’s send some drugs down the spinal cord to block all this talk about danger. And, we’ll make this feel like a “good” pain, not an injury.” The drugs reduce pain and thereby improve movement temporarily.
If the results are only temporary, can there be any progressive benefit? I think the answer is: it depends. Pain relief and improved movement open a window of opportunity that one might climb through. If you are feeling better only for an hour, this provides enough time to train movements that would not normally be accessible, learn new skills, develop new capacities, and reduce the perceived threat associated with certain movements. This could have permanent benefit
sensory • Vigorous pressure placed on the soft tissue may overload the cutaneous receptors, possibily dulling the sensation of the stretch endpoint and increasing stretch tolerance, therefore increasing joint ROM.
Physiological results vs physical results • Is A really caused by B?
At the Physical Level • An acute bout of self myofascial release increase ROM without a subsequent decrease in muscle Activation or force
Force production • No force deficits following foam rolling • Subjects were able to produce similar forces during both conditions and at all time points.
Joint ROM • Significant main effect for the foam roller condition on knee joint ROM. Overall subjects ROM during the control condition was significantly lower, a mean difference of approximately 10 degrees in comparison to the foam roller group. • A post hoc analysis revealed that compared to pre-foam rolling ROM, ROM significantly increased 12.7% and 10.3% at 2 and 10 minutes respectively, post foam rolling.
Resources • http://www.bettermovement.org/2013/how-does-foam-rolling-work/ • http://www.strengthandconditioningresearch.com/2013/10/01/foam-rolling/ • http://saveyourself.ca/articles/does-fascia-matter.php • http://saveyourself.ca/articles/trigger-point-doubts.php
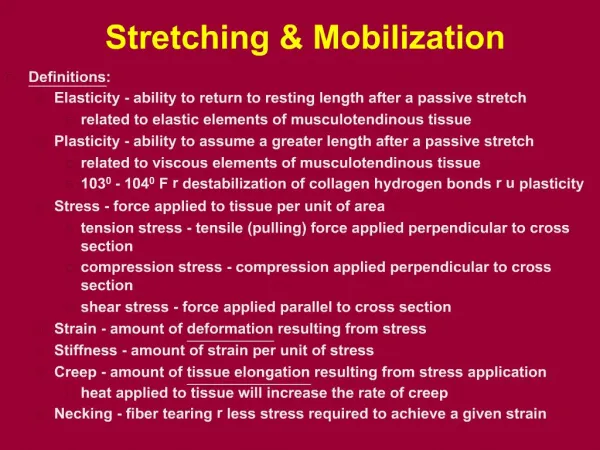
Flexibility • Viscoelastic deformation • Plastic deformation • Increased sarcomere in series • Neuromuscular relaxation • Sensory theory
Viscoelastic deformation • Skeletal muscles are considered to be viscoelastic • Behave elastically- resume original length once tensile force is removed • Behave viscously – response to tensile force is rate and time dependent
An immediate increase in muscle length can occur due to the viscous behavior of muscles whenever they undergo stretch of sufficient magnitude and duration or frequency. This increased length is a viscoelastic deformation because its magnitude and duration are limied by muscles inherent elasticity.
Solid theory? • In human studies the results refute viscoelastic deformation as a mechanism for lasting increases in muscle length and extensibility • All studies consistently showed deformation of human muscle to be transient in nature
Plastic deformation • The classical model of plastic deformation would require a stretch intensity sufficient to pull connective tissue within the muscle past the elastic limit and into the plastic region of the torque/angle curve so that once the stretching force is removed the muscle would remain permanently in a lengthened state.
Solid theory? • No evidence to support it, most citations on the theory can be traced back to a study on rats.
Increased sarcomeres in series • When muscles are immobilized in fully extended positions, there is an increase in the number of sarcomeres in series • When muscles are immobilized in shortened positions there is a decrease in the number of sarcomeres in series and a concurrent decrease in muscle length.
SOLID THEORY? • Too much generalization when comparing immobilization to intermittent static stretching.
Neuromuscular relaxation • In order to increase muscle extensibility, it often been proposed that slowly applied static stretch (used alone or in combination with therapeutic techniques associated with PNF) stimulates neuromuscular reflexes that induce relaxation of muscles undergoing static stretch.
SOLID theory? • Experimental evidence does not support any of these assertions. • Stretch reflexes have been shown to activate during very rapid and short stretches of muscles that are in a mid range position, producing a muscle contraction of short duration. However, most studies of subjects who were asymptomatic and whose muscles were subjected to a long slow, passive stretch into end range positions dud not demonstrate significant activation of stretched muscles.
SENsory theory • increases in muscle extensibility observed immediately after stretching and after short term (3-8 weeks) stretching programs are due to an alteration of sensation only and not to an increase in muscle length. • The change in subjects perception of sensation is the only current explanation for these results.
Subjects may demonstrate an increase in extensibility because they expect this to be the result of stretching. • Increased extensibility then may be due to a psychological alteration in sensory perception or to a willingness of subjects to tolerate greater torque application.
Is passive muscle stiffness necessary to stop joint motion, or is it possible that just the subjects sensory perception of stiffness or perception of moderate stretch can be a limiting factor?