Download
1 / 60
730 likes | 1.81k Vues
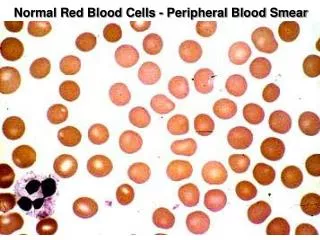
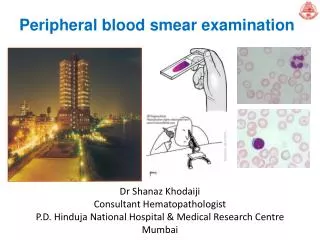
Examination of Peripheral Blood Smear. A well Made and well Stained Smear can provide: . Estimates of cell count Proportions of the different types of WBC Morphology. Peripheral Blood Smear. Objective 1. Specimen Collection 2. Peripheral Smear Preparation

E N D
A well Made and well Stained Smear can provide: • Estimates of cell count • Proportions of the different types of WBC • Morphology
Peripheral Blood Smear • Objective 1. Specimen Collection 2. Peripheral Smear Preparation 3. Staining of Peripheral Blood Smear 4. Peripheral Smear Examination
Specimen Collection • Venipuncture should be collected on an EDTA Tube EDTA liquid form preferred over the powdered form Chelates calcium Disodium or Tripotassium ethylenediamine tetra-acetic acid
Specimen Collection • Advantages • Many smears can be done in just a single draw • Immediate preparation of the smear is not necessary • Prevents platelet clumping on the glass slide
Specimen Collection • Disadvantages: PLATELET SATELLITOSIS • causes pseudothrombocytopenia and pseudoleukocytosis • Cause: Platelet specific auto antibodies that reacts best at room temperature
Specimen Collection • Platelet satellitosis
Specimen Collection • Solution recollect specimen using Sodium Citrate in a 9:1 dilution Correction for dilution 2.7 ml blood 0.3 ml anticoagulant 9/10 dilution is reciprocal 10/9 = 1.1 all computations for WBC and Platelet should be multiplied to 1.1
Peripheral Smear Preparation • Wedge technique • Coverslip technique • Automated Slide Making and Staining
Peripheral Smear Preparation • Wedge technique • Easiest to master • Most convenient and most commonly used technique • Material needed • Glass slide 3 in X 1in • Beveled/chamfered edges
Peripheral Smear Preparation • Procedures: • Drop 2-3 mm blood at one end of the slide Diff safe can be used a. Easy dropping b. Uniform drop
Peripheral Smear Preparation Precaution: Too large drop = too thick smear Too small drop = too thin smear
Peripheral Smear Preparation • The pusher slide be held securely with the dominant hand in a 30-45 deg angle. - quick, swift and smooth gliding motion to the other side of the slide creating a wedge smear
Peripheral Smear Preparation Wedge Technique • Push Type wedge preparation • Pull Type wedge prepartion
Peripheral Smear Preparation Precautions: Ensure that the whole drop of blood is picked up and spread Too slow a slide push will accentuate poor leukocyte distribution, larger cells are pushed at the end of the slide Maintain an even gentle pressure on the slide Keep the same angle all the way to the end of the smear.
Peripheral Smear Preparation Precautions: Angle correction: 1. In case of Polycythemia: high Hct angle should be lowered - ensure that the smear made is not to thick 2. Too low Hct: Angle should be raised
Feature of a Well Made Wedge Smear • Smear is 2/3 or ¾ the entire slide • Smear is finger shaped, very slightly rounded at the feathery edge: widest area of examination • Lateral edges of the smear visible • Smear is smooth without irregularities, holes or streaks • When held up in light: feathery edge should show rainbow appearance • Entire whole drop of blood is picked up and spread
Peripheral Smear Preparation • Cover Slip Technique rarely used used for Bone marrow aspirate smears Advantage: excellent leukocyte distribution Disadvantage: labeling, transport, staining and storage is a problem
Peripheral Smear Preparation • 22 x 27mm clean coverslip • More routinely used for bone marrow aspirate • Technique: 1. A drop of marrow aspirate is placed on top of 1 coverslip 2. Another coverslip is placed over the other allowing the aspirate to spread. 3. One is pulled over the other to create 1 thin smears
Peripheral Smear Preparation 4. Mounted on a 3x1 inch glass slide Precautions: • Very lgiht pressure should be applied between the index finger and the thumb • Crush preparation technique • Too much pressure causes rupture of the cells making morphologic examination impossible • Too little pressure prevents the bone spicules from spreading satisfactorily on the slide
Peripheral Smear Preparation • Automatic Slide Making and Staining • SYSMEX 1000i
Peripheral Smear Preparation • Drying of Smears Fan Heating pans No breath blowing of smears – may produce crenated RBCs or develop water artifact (drying artifact)
Staining of Peripheral Blood Smear • Wright Staing Method • Automated Slide Stainers • Quick Stains
Staining of Peripheral Blood Smear • Pure Wright stain or Wright Giemsa stain • Blood smears and bone marrow aspirate • Polychrome stains: Eosin and Methylene blue stains • Purpose: see and evaluate cell morphology
Staining of Peripheral Blood Smear • Eosin + Methylene Blue = thiazine eosinate complex • The complex will not stain any color unless a buffer is added: 0.05M sodium phosphate (pH 6.4) and aged distilled water (pH 6.4-6.8) • Methanol is added to fix the cells on the slide
Staining of Peripheral Blood Smear • Free Methylene Blue: - basic - stains acidic cellular components such as RNA • Free Eosin - acidic - stains basic cellular components such as Hgb and eosinophilic granules
Staining of Peripheral Blood Smear • Problem encountered during staining Water artifact: moth eaten RBC, heavily demarcated central pallor on the RBC surface, crenation, refractory shiny blotches on the RBC
Staining of Peripheral Blood Smear • What contributes to the problem: • humidity in the air as you air dry the slides. • Water absorbed from the humid air into the alcohol based stain • Solution: • Drying the slide as quickly as possible. • Fix with pure anhydrous methanol before staining. • Use of 20% v/v methanol
Staining of Peripheral Blood Smear • AUTOMATED SLIDE STAINERS • It takes about 5-10 minutes to stain a batch of smears • Slides are just automatically dipped in the stain in the buffer and a series of rinses • Disadvantages: • Staining process has begun, no STAT slides can be added in the batch • Aqueous solutions of stains are stable only after 3-6 hours
Staining of Peripheral Blood Smear HEMA-TEK STAINER
Staining of Peripheral Blood Smear • QUICK STAINS • Fast, convenient and takes about 1 minute to be accomplished • Modified Wrights-Giemsa Stain, buffer is aged distilled water • Cost effective • Disadvantage: Quality of stains especially on color acceptance For small laboratories and for physician’s clinic only
Features of a well-stained PBS • Macroscopically: color should be pink to purple • Microscopically: RCS: orange to salmon pink WBC: nuclei is purple to blue cytoplasm is pink to tan granules is lilac to violet Eosinophil: granules orange Basophil: granules dark blue to black
Features of a well-stained PBS • Troubleshooting: • RBC gray, WBC too dark Eosinophil granules are gray Cause: stain or buffer is to alkaline inadequate rinsing Prolonged staining heparinized sample
Features of a well-stained PBS • Troubleshooting: • RBC too pale, WBC barely visible Causes: Stain or buffer is too acidic Underbuffering Over rinsing
Peripheral Smear Examination • Macroscopic • Overall bluer color: increased blood proteins (multiple myeloma, rouleaux formation) • Grainy appearance: RBC agglutination (cold hemagglutinin diseases) • Holes: increased lipid • Blue specks at the feathery edge: Increased WBC and Platelet counts
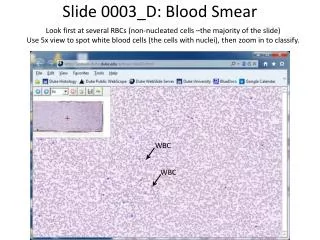
Peripheral Smear Examination • Microscopic: • 10x Objective • Assess overall quality of the smear i.e feathery edge, quality of the color, distributin of the cells and the lateral edges can be checked for WBC distribution • Snow-plow effect: more than 4x/cells per field on the feathery edge: Reject • Fibrin strands: Reject • Rouleaux formation, large blast cell assessment
Peripheral Smear Examination • Microscopic: • 40x Objective • Correct area where to star counting is determined • WBC estimate: internal quality control
Peripheral Smear Examination • Microscopic: • 100x Objective; OIO • Highest magnification • WBC differential counting
Peripheral Smear Examination • Optimal Assessment Area: • RBCs are uniformly and singly distributed • Few RBC are touching or overlapping • Normal biconcave appearance • 200 to 250 RBC per 100x OIO
Peripheral Smear Examination • Too thin • Too thick
Performance of a White Blood Cell Differential Count • Systematic • Choose the best area for assesment • Back and forth serpentine or battlement track patters in preferred
Performance of a White Blood Cell Differential Count • 100 WBCs are counted using a push down counters (Clay Admas Laboratory counters,Biovation diff counters • Accuracyof Diff Count: Count 200 WBC if WBC>40 x 109/L Extremely low WBC counts, do the Diff count under 50X OIO
Performance of a White Blood Cell Differential Count • Extremely low WBC counts, do the Diff count under 50X OIO • Extremely low WBCs: WBC are concentrated, buffy coat smears are made
RBC Morphology Anisocytosis Poikilocytosis Cellular Inclusions
Platelet Estimate • Choose an area where RBC barely touch • No. of platelet in 10 OIO fields is counted multiplied by 20,000 • Anemia or Erythrocytosis • Average No. of Plts/field x total RBC count 200 RBCs/field (200 is the average number of RBC/field)
Summarizing WBC parameters • Total WBC counts per (WBC x 109/L) • WBC differential counts are percentages • WBC differential count values expressed as actual number of each type of cell • WBC morphology
Summarizing WBC parameters • STEP 1 WBC increased : leukocytosis WBC decreases: leukopenia