Nursing Perceptions of Optimal Pain Management in Pediatric Patients
10 likes | 82 Vues
This study explores how nurses working with pediatric patients define and approach optimal pain management. Results reveal differences between critical care and acute care units in defining optimal pain management. The study highlights the importance of understanding nurses’ perspectives to enhance pediatric pain management practices.

Nursing Perceptions of Optimal Pain Management in Pediatric Patients
E N D
Presentation Transcript
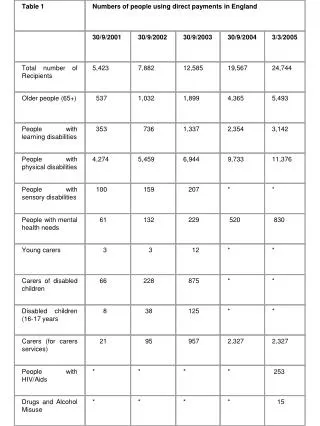
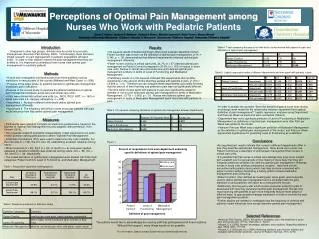
Perceptions of Optimal Pain Management among Nurses Who Work with Pediatric Patients Susan T. Heinze¹, Gustavo R. Medrano¹, Katherine Simon¹, Michelle Czarnecki², Helen Turner³, Sharon Wrona4 University of Wisconsin-Milwaukee¹, Children’s Hospital of Wisconsin², Doernbecher Children's Hosptial³, Nationwide Children's Hospital4 Introduction Compared to other age groups, children may be at risk for poor pain management (American Pain Society, 2003). Unfortunately, there has been limited research on pain management in pediatric populations (Vincent, 2005). In order to help children receive the pain management that they are entitled to, it is important to understand how nurses view optimal pain management for pediatric patients. • Results • Chi-squared results indicated significant differences between department when Patient Comfort was chosen as the definition of optimal pain management, χ² (1) = 6.345, p < .05, demonstrating that different departments endorsed optimal pain management differently. • Fewer nurses working in critical care units, 24.7% (n = 47) defined optimal pain management as Patient Comfort compared to 35.0% (n = 153) of nurses in acute care units. Nurses in critical care and acute care units defined optimal pain management similarly in terms of Level of Functioning and Medication Management. • Preliminary results of a Chi-squared indicated that departments did not differ significantly in the amount of time that they worked with patients in pain, χ² (10) = 14.908, p = ns. Therefore we can compare these departments accurately, knowing that the amount of time that they see patients in pain was not significantly different. • The time which nurses spent with patients in pain was significantly related to whether or not a nurse described optimal pain management in terms of Medication Management, t (770) = -2.609, p < .01. Nurses who defined optimal pain management in terms of Medication Management spent more time with patients in pain. Table 4. T-test comparing the amount of time which nurses worked with patients in pain and definitions of optimal pain management Table 5. Logistic regression model of different departments and time spent with patients in pain • Methods • A multi-site investigation surveyed nurses from three pediatric nursing institutions in various parts of the country (Midwest and West Coast; n = 808). • Purpose of the larger study: to examine barriers to optimal pain management in pediatric pain institutions. • Purpose of the current study: to examine the different definitions of optimal pain management between acute care and critical care units. • Units were divided into critical care units (i.e., NICU, PICU, HOT; n = 190) or acute care units (i.e., surgery, emergency; n = 438). • Hypothesis 1: Nurses in different units would define optimal pain management differently. • Hypothesis 2: The frequency with which nurses encounter patients with pain would influence how they define optimal pain management. • In order to answer the question “Does the amount of pain a nurse sees during an average week moderate the relationship between department and optimal definition of pain management?” logistic regression analyses using Department and Pain per Week as predictors were conducted (Table 5). • Department was not a significant predictor of Level of Functioning or Medication Management as definitions of optimal pain management even after Pain per Week was added to the model. • However Pain per Week was a significant predictor of Medication Management as the definition of optimal pain management in this model, and Pain per Week approached significance for predicting Level of Functioning as a definition. Table 3. Chi-squared comparing definitions of optimal pain management between departments • Measures • Participants were asked to complete an electronic questionnaire, based on the Barriers to Optimal Pain Management survey adapted, with permission, from Vincent (2004). • Two graduate research assistants independently coded responses to an open-ended question asking participants to define “Optimal Pain Management”. • IntraClass Correlations (ICC) were used to determine inter-rater reliability. For the first code (n = 136), the ICC was .96, establishing excellent reliability among raters. • When a second (n = 90), third (n = 34), or fourth (n = 9) code were needed, adequate to excellent reliability was observed among raters, ICC = .88, ICC = .86, and ICC = .99, respectively. • The coded definitions of optimal pain management were divided into three main categories: Patient Comfort, Level of Functioning, and Medication Management. • Conclusions • As hypothesized, results indicate that nurses in different departments differ in how they describe optimal pain management. More acute care nurses use Patient Comfort as a descriptor of optimal pain management than nurses in critical care units. • It is possible that that nurses in critical care settings may have more contact with a patient over longer periods of time making it more likely that they will integrate additional variables into defining optimal pain management. Whereas nurses in acute care settings (emergency, surgery), may have shorter encounters with patients during which they may be more concerned with patient comfort without developing a history which involves medication management and functioning. • Patient Comfort, often defined as meeting pain score goals, was frequently used to define optimal pain management and is consistent with the gold standard of using patients' self report as a measurement for pain. • Additionally, the frequency with which nurses encounter patients in pain is associated with how they perceived optimal pain management. Nurses who report working with patients in pain more frequently may be more aware of different ways to appropriately manage medication in order to provide the best pain management possible. • Further studies are needed to investigate how the frequency of working with patients in pain influences how nurses describe optimal pain management. Figure 1. Table 1. Respondent department demographics Table 2. Response examples for definition codes • Selected References • American Pain Society. (2003). Principles of analgesic use in the treatment of acute pain and cancer pain. (5th ed.) Glenview, IL: Author. • Vincent, C.V. (2005). Nurses’ knowledge, attitudes, and practices: Regarding children’s pain. MCN, 30(3), 177-183. • Vincent, C.V. & Denyes, M.J. (2004). Relieving children’s pain: Nurses’ abilities and analgesic administration practices. Journal of Pediatric Nursing, 19(1), 40-50. For information, please contact Susan Heinze at stheinze@uwm.edu