Download
1 / 42
420 likes | 579 Vues
Preventing Athletic Injuries. Tony Milian, ATC, LAT Manager, Sports Medicine [U18] Sports Medicine Cooper City Optimist Lecture February 16th, 2010. Parents’, Coaches’, Trainers’, Physicians’ Everybody’s Goals. Make the game as safe as possible for the players

E N D
Preventing Athletic Injuries • Tony Milian, ATC, LAT • Manager, Sports Medicine • [U18] Sports Medicine • Cooper City Optimist Lecture • February 16th, 2010
Parents’, Coaches’, Trainers’, Physicians’Everybody’s Goals • Make the game as safe as possible for the players • Protect the athlete from further injury • Accurate evaluation • Early recognition and treatment • Definitive injury care • Return to play
Prevention • Representative Areas For Today: • Head Injury • Heat Injury • Supplement Injury • Lightning Injury • Stretching Dynamic / Static
Head Injury: Concussion • Definition - Immediate and transient impairment of neurologic function due to traumatic injury to the head • May or may not involve loss of consciousness (LOC)
Early Signs of Concussion • Impaired attention • Slurred, incoherent speech • Disorientation • Impaired Coordination • Emotional reaction out of proportion • Memory deficits • Any loss of consciousness
Late Signs of Concussion • Persistent headache • Dizziness • Poor Attention • Memory Dysfunction • Nausea or Vomiting • Irritability • Photophobia
AAN Concussion Grading Scale • Grade I • Abnormal symptoms resolve in less than 15 minutes • Grade II • Abnormal symptoms resolve in greater than 15 minutes • Grade III • A: Brief LOC (seconds) • B: Prolonged LOC (minutes)
Assessment • Cervical Spine (LOC) • Facial Expression • Pupil size and reactivity • Upper and Lower extremity • Orientation • Immediate Memory • Delayed Recall
AAN Concussion Management • Grade I (<15 minutes, no LOC) • Remove from contest • Immediate exam and at 5 minute intervals • Out for Remainder of Game
AAN Concussion Management • Grade II (>15 minutes, no LOC) • Remove from contest; no return • Immediate exam and at 5 minute intervals • Re-exam the next day • MD exam and clearance after 1 asymptomatic week
AAN Concussion Management • Grade III (Any LOC) • EMS transport to nearest ER • MD evaluation and +/- brain imaging • Possible Admit
AAN Concussion Management • Grade III - Return to play • Brief LOC : 1 week • Prolonged LOC : 2 weeks • 2nd Injury: 1 month • Abnormal Brain Scan : season terminated
Heat Injury • When “walk it off” is not the right thing to say • What three types exist • What are the risk factors • Prevention strategies • Treatment strategies • Heat cramps • Heat exhaustion • Heat stroke
Heat Related Injury • Heat production increases 15X with exercise • Two mechanisms to dissipate head • Radiation (65%) – Clothing • Evaporation (30%) – Humidity
Heat Related Injury • Heat Cramps • Painful muscle spasms that most commonly occur in the calf and abdomen but can occur anywhere. • Treatment involves drinking water, mild stretching and ice massage of the affected area.
Heat Related Injury • Heat Exhaustion • Headache • Dizziness • Weakness • Fatigue • Muscle cramps • Vomiting • Excessive thirst dry tongue and mouth • In-coordination, mental dullness, • Elevated body temperature & reduced sweating. Looks Like a Viral Illness
Heat Related Injury • Heat Exhaustion • Treatment • Rest • Remove from hot environment • Fluid replacement over several hours • Likely requiring IV fluid • Ice packs to neck, groin, armpits
Heat Related Injury • Heat Stroke • Sudden collapse usually with a loss of consciousness • Flushed, hot skin; Rapid, strong pulse • Sweating is often absent • Body has lost the ability to cool itself • Treatment - Immediate call to 911 and • Cool the body • Strip all the clothing off the athlete • Sponge with cool water, and fan with a towel • Ice water immersion is controversial • No alcohol sponge baths
Heat Related Injury • Prevention Strategies • Education • Hydration • Prior to activity (1/2 liter starting 2 hours prior to activity) • Every 15-20 minutes during activity • If Child = 5oz • If Adolescent = 9oz • Rest • More frequently during hot and humid days • Schedule adjustment • Equipment removal
Heat Related Injury • Hydration • Sports Beverages Recommended • Carbohydrate (glucose and sucrose) • Sodium • Potassium
Heat Related Injury • WARNING!!!
Heat Illness • Heat illness may be hard to detect • Fluids before / during / after • EMS activation • Treatment on scene • Prevention is key
Supplement Illness • Caffeine • Steroids • GNC • Amphetamines • Red Bull
Caffeine Content Standard 4 ounce cup = 50 mg caffeine 8 oz Red Bull 16 oz Rockstar 16 oz Arizona 8 oz Cocaine Energy Drink OR 2 oz Extreme Energy
Lightning Injury • Florida ranks as # 1 in the US for lightning related injury and death • One out of every 9 lightning strikes end in a fatality • Common misconceptions
Lightning • Lightning strikes up to 25 miles away • Be Proactive! • Plan Ahead • Monitor the weather • Postpone the activity • Get to a safe place
Lightning • Use the 30/30 rule… • If time between lightning and thunder is LESS than 30 seconds…get to a safe place!!! • WAIT 30 seconds after hearing last thunder before leaving safe location • Retreat to an enclosed building • Vehicle with closed window adequate • OK to touch victim • AVOID… • Dugout • Picnic pavilion • Rain shelter
Lightning • Move victim ONLY if necessary, with particular attention to any possible brain or spinal cord injury • Examine for burns, broken bones, cuts, loss of hearing or eyesight • Emergency Plan Activation • Activate your plan • Notify EMS • AED if available • Log roll • Initiate effective CPR
Some Emergencies on the field Obviously need 911 • Dislocations • Open Fractures • Gross Deformities • LOC
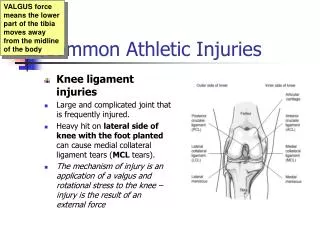
Injury Prevention • 3.5 million injuries each year • Most common are strains and sprains • Prevention • Dynamic warm up • Static stretching • Proper biomechanical training 33
Stretching • Stretching: the act of performing a particular exercise to improve joint range of motion. European College of Sports Sciences 2006. • Static Stretching: when a body part is taken to a point of mild discomfort and held for an amount of time. • Dynamic Stretching/Movements: movements that maximize active range of motion and elevate core body temperature. • Journal of Strength and Conditioning 2005 34
Static vs. Dynamic • Does static stretching prior to activity achieve the goals of injury prevention and performance enhancement? • NO • Research has shown that static stretching can be detrimental to performance and does not lead to a decrease in injury 35
Static vs. Dynamic • Study from the Journal of Strength and Conditioning, 2008 • 24 Division I wrestlers were randomly assigned to complete a 4 week Dynamic or Static warm up routine prior to their preseason practices • 11 performed the static warm up • 13 performed the dynamic warm up • They were tested on med ball underhand throw, 300 yard shuttle, pull ups, push ups, sit ups, broad jump, 600 m run, sit to stand reach, trunk extension, quad and hamstring peak torque tests. 36
Static vs. Dynamic • Results Dynamic Group • Increase in quadriceps peak torque by 11% • Increase in broad jump by 4% • Increase in underhand med ball throw by 4% • Increase in sit ups by 11% • Increase in push ups by 3% • Static group posted no improvements to tests performed. 37
Static vs. Dynamic • Study from the Journal of Strength and Conditioning, 2006 • United States military academy took 30 cadets to do a study on static vs. dynamic warm up routines to see which one would better prepare their cadets for power and agility activities • Tested on the 5 step jump to determine functional leg power • Medicine ball throw was chosen to measure total body power • T-drill was chosen to measure agility 38
Static vs. Dynamic • For 3 days one group of cadets performed static stretches for 10 minutes prior to data collection • Other group performed dynamic stretches for 10 minutes • All routines were done at 6AM each day • There was a 2 minute period between finishing the warm up and beginning the performance test 39
Static vs. Dynamic • Results • T –drill static warm up = 9.69 sec vs. dynamic’s 9.56 sec • Medicine ball throw = 9.34 meters with static vs. 9.79 meters with dynamic • 5 step jump = 9.78 meters with static vs. 10.06 meters with dynamic • For task requiring power and agility, the results suggest that dynamic warm up will offer performance benefits not found with static warm ups. 40
Thank YouTony Milian, ATC, LATManager, [U18] Sports Center954-538-5501amilian@mhs.netwww.u18sportsmedicine.com