LIVER
LIVER. By Michael Brillantes, MD, FPCS, FPSGS. Anatomy -1/50 of total body weight. Surgically divided into the right and left lobe by a line through the IVC and gallbladder (Cantlie’s line). -left lobe divided into medial and lateral segments by falciform ligament.

LIVER
E N D
Presentation Transcript
LIVER By Michael Brillantes, MD, FPCS, FPSGS
Anatomy • -1/50 of total body weight • Surgically divided into the right and • left lobe by a line through the IVC and • gallbladder (Cantlie’s line)
-left lobe divided into medial and lateral segments by falciform ligament -blood supply hepatic a. - 25% portal v – 75%
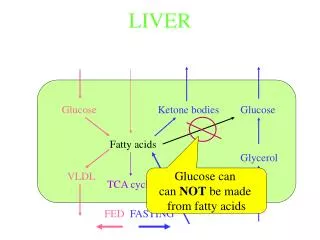
II. Liver function • Circulatory function- material absorbed from the GI tract are brought to the liver through the dual blood supply to be used in the metabolic pool
B. Biliary passages- channel of exit for materials secreted by the liver through the dual blood supply to be used in the metabolic pool
C. Reticuloendohelial system- contains phagocytic Kupffer cells and endothelial cells D. Metabolic Activity- anabolic and catabolic activities
III. Function Tests a. Albumin – half- life is 21 days; decrease means a chronic liver disease (more than 3 wks)
B. Carbohydrates and Lipids- hepatic disease causes decrease in glycogenesis with resultant hyperglycemia
C. Enzymes • Alkaline phospatase- increase indicates • an obstructive pathology
2. SGOT and SGPT- increase indicates liver cellular damage; SGPT more applicable for hepatic disease 3. Dye excretion
4. Coagulation factors a. Vit. K dependent clotting factors II, VII, IX, and X b. Inability to synthesize prothrombin
IV. Special Studies A. Needle Biopsy- provides pathologic diagnosis B. Ultrasound, CT scan, MRI C. Angiography
V. Pathology • Trauma- 2nd most commonly injured organ • 1. Clinical manifestation- shock, abdominal pain, spasm, and rigidity
2. Diagnostic- CT scan is the most useful - may also use ultrasound, paracentesis or peritoneal lavage
3. Treatment • Correct shock- IVF and blood • Surgery • Control bleeders- perihepatic packaging, ligation of bleeders, Pringle maneuver • Debridement • External drainage
4. Complications • Recurrent bleeding- inadequate homostasis or loss of coagulation factors secondary to massive transfusions • Intraabdominal sepsis
C. Hematobilia- free communication between blood vessel and biliary tree - triad of abdominal pain, GI bleeding, and previous trauma - jaundice may be present
B. Hepatic Absdess 1. Pyogenic- most commonly due to cholangitis secondary to CBD obstruction; septicemia second most common etiology
- Fever with “picket fence” pattern, hepatomegally and tenderness -organism- usually e. coli -usually found in the right lobe, solitary or multiple
Presents with hepatic tenderness and fever • Diagnostic • i. CBC- leukocytosis, with count up to 18-20,000
ii. Radiograph- immobility or elevation of right hemidiaphragm iii. Ultrasound or CT scan
b. Treatment I .Antibiotics- IV for 2 wks, followed by 1 month oral form II. Drainage- percutaneous under ultrasound or CT guidance, or open
2. Amebic- reaches the liver via the portal vein from an ulceration in the bowel wall -organism- e. histolytica -occurs in the right lobe, usually solitary, with characteristic “anchovy paste”
Fever and liver pain, assoc. woth tender hepatomegally • 33% with antecedent diarrhea
Diagnostic • i. CBC- leukocytosis • ii. Indirect heme agglutinstion test • iii. Ultrasound • iv. Aspiration of trophozoites
b. Complications i. Secondary bacterial infection ii. rupture
c. Treatment i. Amebicidal drugs- Metronidazole 500 mg TID ii. Surgery – indicated for persistence of abscess, secondary infection
C. Cysts 1. Non- parasitic – usually solitary, found in the right lobe, watery content, with low internal pressure
-polycystic liver assoc. with polycystic kiny in 51.6% of cases -usually presents as a RUQ mass
Classification • Blood or degenerative • Dermoid • Lymphatic • Endothelial • Retention – polycystic liver • Proliferative cysts- cystadenomas
b. Diagnostic – ultrasound, CT scan, arteriography, scintillography, peritoneoscopy c. Asymptomatic- no treatment Symptomatic- drainage with unroofing or sclerotherapy
2. Hydatid cysts- caused by Echinococcus granulosus - with high internal pressure, causing rupture and anaphylactic reaction
Asymptomatic unless there are pressure symptoms on adjacent organs • Diagnostic- radiograph, ultrasound and CT scan • -Casoni’s skin test
b. Treatment i. small calcified cyst- no treatment ii. Sterilizationof cyst prior to surgery with hypertonic saline or alcohol followed by surgical removal
D. Benign Tumors 1. Classification a. Hamartomas- tissues normally found in the organ but arranged in a disorderly manner
b. Adenoma- associated with contraceptive use; may transform into hepatocellular carcinoma; high rate of bleeding
c. Focal nodular hyperplasia- reaction to injury or a response to a preexisting vascular malformation d. Hemangioma- most common nodule in the liver
2. Diagnostic- ultrasound, CT scan, angiography 3. Treatment- excision if symptomatic
E. Malignant lesions 1. Primary carcinoma- from Aspergillus flavus, kwashiorkor
Classification • hepatoblastoma- usually affects children less than 2 years old.
ii. Fibrolamellar carcinoma- adolescent and young adults; large solitary lesion iii. Hepatocellular carcinoma- most common primary malignancy, usually follows postnecrotic cirrhosis (hepatitis B)
Manifested by mass, weight loss, abdominal pain, or intraperitoneal hemorrhage
b. Diagnostic i. Liver function test- alkaline phosphatase ii. Alpha Feto Protein
iii. Angiography iv. Ultrasound, intraoperative ultrasound, CT scan, MRI
c. Treatment- curative resection, chemotherapy with direct arterial infusion
2. Other Primary Neoplasms • Sacroma- angiosacroma most common • Mesenchymoma • Infantile hemangioendothelioma
3. Metastatic neoplasms - most common malignant tumor of the liver - reach the liver by portal vein, hepatic artery, lymphatics, direct extension
Symptoms are usually referable to the liver (i.e. pain, ascites, weight loss, anorexia and jaundice
Diagnostic • i. alkaline phosphatase • ii. Serum marker referable to the primary carcinoma • iii. SGOT • iv. CT scan, MRI
b. Treatment • Control primary tumor • Check for other systemic metastases • Patient should be able to tolerate a major resection • Resection of metastasis should be feasible