
Liver Histology and Functions: A Comprehensive Overview
Explore liver histology, bile production, hepatic artery, portal vein, and liver zones. Learn about liver function, enzyme production, detoxification, and classification of jaundice. Discover causes, types, and clinical features of liver disease.

Liver Histology and Functions: A Comprehensive Overview
E N D
Presentation Transcript
HISTOLOGY BILE DUCT HEPATIC ARTERY PORTAL VEIN ZONE 1 ZONE 2 ZONE 3 CENTRAL VEIN
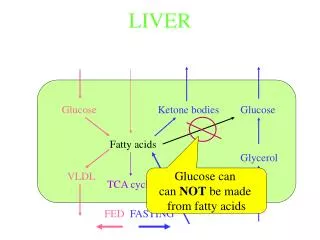
LIVER FUNCTION • SYNTHESIS • Albumin, clotting factors, fibrinogen, complement, alpha1-antitrypsisn • ENZYME PRODUCTION • AST, ALT, GT, Alk phos • DETOXIFICATION • METABOLISE DRUGS • BILE PRODUCTION
CLASSIFICATION OF JAUNDICE • PRE-HEPATIC • heamolysis • INTRA-HEPATIC • hepatitis, cirrhosis, congenital hyperbiliruniaemia • POST-HEPATIC • gallstones, tumours, strictures, biliary atresia Unconjugated bilirubin Conjugated bilirubin (water soluble)
CAUSES OF LIVER DISEASE ORGANISMS TOXINS TUMOURS GALLSTONES
TYPES OF LIVER DISEASE • ACUTE (cell necrosis + inflammation) • virus, alcohol, drugs, gallstones • CHRONIC (continued inflammation) • chronic hepatitis (viruses, alcohol, drugs, autoimmune) • iron overload (Haemochromatosis) • Wilson’s disease • alpha1-antitrypsin deficiency
CLINICOPATHOLOGICAL FEATURES ACUTE CHRONIC • MALAISE • HEPATOMEGALY • JAUNDICE • RAISED BILIRUBIN • RAISED TRANSAMINASES • RECOVERY • LIVER FAILURE - if severe • CHRONIC DISEASE • ASYMPTOMATIC • CIRRHOSIS • PORTAL HYPERTENSION • oesophageal varices • LIVER FAILURE • oedema, ascities, coma • HEPATOMA
CIRRHOSIS - MORPHOLOGY MICRONODULAR <3MM (commonest cause is alcohol) MACRONODULAR >3MM (greater risk of carcinoma)
Diffuse Hepatomegally • Inflammation • Parasite------hydatid • Protozoal -------- amaobic, kala azar • Pyogenic ---- pyogenic liver abcess • Bacterial -----miliary TB , typhoid, Brucelosis • Viral ----- infective hepatitis, yellow fever • Spirochetal syphilis • Richetsial ----- typhus
Diffuse Hepatomegally • Blood diseases • Anaemias • Leukemias • Lymphoma • Liver congestion • Budd chiarri • Tricusped stenosis • Constrictive pericarditis • Right heart failure • Veno-occlusive disease
Diffuse Hepatomegally • Liver cirrhosis • Cardiac • Biliary • Early stages of othes • Liver tumors • HCC • Secondaries • Metabolic • Fatty liver • Gaucher’s (lipoid storage) • Von Gierki’s disease ( gycogen storage) • Amyloidosis
Localized Hepatomegally • Cystic • Hydatid liver cyst • Amoebic liver abscess • Solid • Congenital ------ Riedel’s lobe • Tumors • Benign ----- haemangioma • Malignant • HCC • Secondaries
Hepatic Cysts • The term hepatic cyst usually refers to solitary non-parasitic cysts of the liver, also known as simple cysts. • Most patients with simple cysts are asymptomatic and require no treatment. • When the cysts become large and cause symptoms such as pain, treatment is warranted. • Today, laparoscopic unroofing of large simple cysts has become the preferred treatment option.
The cause of simple liver cysts • The cause of simple liver cysts is unknown, but cysts are believed to be congenital in origin. • The cysts are lined by biliary-type epithelium and perhaps result from progressive dilatation of biliary microhamartomas. • Because liver cysts seldom contain bile, the current hypothesis is that the microhamartomas fail to develop normal connections with the biliary tree.
DD of cystic lesions • Congenital • Simple cysts • multiple cysts arising in the setting of congenital polycystic liver disease • Traumatic • Hematoma • Biloma • Parasitic or hydatid (echinococcal) cysts • Abscesses. • Pyogenic • Amoebic • Cystic tumors • Benign • malignant
liver cysts • Simple cysts generally cause no symptoms or produce right upper quadrant pain and have a typical radiographic appearance. • Polycystic liver disease can arise in childhood or adult life as part of a congenital disorder associated with polycystic kidney disease. • Hydatid cysts are caused by infection with the tapeworm Echinococcus granulosus.
Liver Abscess Direct by Empyema thoracis Subphrenic abcess Penetrating lesion cholecystitis Empyema thoracis Subphrenic abcess Penetrating lesion Hepatic artery cholecystitis Portal vein Biliary umbilicus
Pyogenic liver abscess (Etiology) • Biliary disease • Biliary disease accounts for 21-30% of reported casesusually • Associated with choledocholithiasis, • Benign and malignant tumors, • Postsurgical strictures. • Biliary-enteric anastomoses • Infection via the portal system (portal pyemia) • Hematogenous (via the hepatic artery) • No evident cause
Microbiology: The most common microorganisms isolated from blood and abscess cultures are as follows: • Escherichia coli - 33% • Klebsiella pneumoniae - 18% • Bacteroides species - 24% • Streptococcal species - 37% • Microaerophilic streptococci - 12%
Pyogenic liver abscess • The right hepatic lobe is affected more often than the left by a factor of 2:1. • Bilateral involvement is seen in 5% of cases. • The predilection for the right lobe can be attributed to anatomic considerations. • The right hepatic lobe receives blood from both the superior mesenteric and portal veins. • whereas the left lobe receives inferior mesenteric and splenic drainage. • It also contains a denser network of biliary canaliculi.
Symptoms Young, 70 % male • Fever • Chills • Vomiting & anorexia in 1/3 of cases • Abdominal pain • Weight loss
Signs • Right upper quadrant tenderness • Hepatomegaly • Normal abdominal findings • Jaundice and is usually associated with biliary tract disease or the presence of multiple abscesses. • Chest findings: Decreased breath sounds in the right basilar lung zones, with signs of atelectasis and effusion
Complications • Recurrent septicemia • Extension and rupture may occur in • Peritoneal cavity • general peritonitis or • subphrenic collection • Through the diaphragm~> empyema thoracis
Signs of complications • Signs of peritoneal irritation, such as • rebound tenderness, guarding, and • absence of bowel sounds, are present when the abscess ruptures in the peritoneal cavity. • Peritonitis occurs in 2-7% of cases. • Pericardial friction rub can be audible when the abscess extends into the pericardium. This sign is associated with very high mortality. • Signs of pleural effusion are present when the abscess ruptures in the pleural cavity.
Lab Studies: • Complete blood cell count • Anemia is observed in 50-80% of patients. • Leukocytosis of more than 10,000/mm3 in 75-96% of patients. • Liver function tests • An elevated alkaline phosphatase level in 100% of patients. • An elevated aspartate aminotransferase level • An elevated alanine aminotransferase level, • An elevated bilirubin level is observed in 50% of patients. • Prothrombin time: This is elevated in 80% of patients
Diagnosis • Plain X ray • detect gas in the abscess cavity • Chest basal collapse & sympathetic effucsion • Elevation of diaphragmatic copula • U/S and CT with enhancement are the two mostly used diagnostic accurate methods. • Liver scan by rose bengal or radio-active colloidal gold ( less use) • Angiography ( invasive so less use)
Treatment Medical therapy: • The most dramatic change in the treatment of pyogenic liver abscess has been the emergence of CT-guided drainage. • Prior to this modality, open surgical drainage was the treatment most often employed, with mortality rates as high as 70%. • The current approach includes 3 steps. • Initiation of antibiotic therapy • Diagnostic aspiration and drainage of the abscess • Surgical drainage in selected patients
Treatment Antibiotic therapy • Regimens using beta-lactam/ beta-lactamase inhibitor combinations or • Second-generation cephalosporins with anaerobic are excellent empiric choices for the coverage of enteric bacilli and anaerobes. • Metronidazole or clindamycin should be added for the coverage of Bacteroides fragilis if other employed antibiotics offer no anaerobic coverage. • If fungal pathogens are a possibility, empiric anti-fungal therapy should be considered. Initial therapy for fungal abscess is currently amphotericin B.
Treatment Duration of treatment has always been debated. • Currently 4-6 weeks of therapy is recommended for solitary lesions that have been adequately drained. • Multiple abscesses are more problematic and can require up to 12 weeks of therapy. • Both the clinical and radiographic progress of the patient should guide the length of therapy
Surgery The 5 indications for open surgical drainage are as follows: • Abscess not amenable to percutaneous drainage • secondary to location, and/or • the presence of a complicated, • multiloculated, thick-walled abscess with viscid pus. • Coexistence of intra-abdominal disease that requires operative management e.g. peritonitis • Failure of antibiotic therapy • Failure of percutaneous aspiration • Failure of percutaneous drainage
Surgery • A transperitoneal approach allows for abscess drainage and abdominal exploration • Anterior ----- RT sub-costal approach • Posterior ---- extra-pleural extraperitoneal , through the bed of the last rib
Amoebic liver abscess • Amebic liver abscess is the most frequent extra-intestinal manifestation of Entamoeba histolytica infection. • This infection is caused by the protozoa E histolytica, which ascends the portal venous system. • Amebic liver abscess is an important cause of space-occupying lesions of the liver, mainly in developing countries.
Amoebic liver abscess • The right lobe of the liver is more commonly affected than the left lobe. • This has been attributed to the fact that • the right lobe is supplied predominantly by the superior mesenteric vein, • whereas the left lobe is supplied by the splenic vein. • The pus is usually chocolate colored due to lyses of hepatocytes and RBCs.
Clinically • The signs and symptoms of amebic liver abscess often are nonspecific, resembling those of • pyogenic liver abscess or • other febrile diseases. • There is an acute onset of • fever with rigors and • abdominal pain which comes out of the blue with short duration
Clinically • Young age. • The pain most frequently is located in the right upper quadrant and may radiate to the right shoulder or scapular area. • Pain increases with coughing, walking, and deep breathing, and it increases when patients rest on their right side. • The pain usually is constant, dull, and aching. • Jaundice (<10% of cases) mostly occurs in complicated cases with multiple abscesses or a large abscess compressing the biliary tract.
Signs of complications • Signs of peritoneal irritation, such as • rebound tenderness, guarding, and • absence of bowel sounds, are present when the abscess ruptures in the peritoneal cavity. • Peritonitis occurs in 2-7% of cases. • Pericardial friction rub can be audible when the abscess extends into the pericardium. This sign is associated with very high mortality. • Signs of pleural effusion are present when the abscess ruptures in the pleural cavity.
Course and complications Resoltion rupture Dormant abscess Secondary infection calcification Destroy liver architecture
Lab Studies: • Approximately three fourths of patients with an amebic liver abscess have leucocytosis mainly eosiophilia. • Serology detect by IHAT • Stool detect E histolytica
Imaging Studies: • Plain X ray • detect gas in the abscess cavity • Chest basal collapse & sympathetic effucsion • Elevation of diaphragmatic copula • Ultrasonography is the preferable initial diagnostic test. • It is rapid, has a low cost, and is only slightly less sensitive than CT scan. • The lesions tend to be round or oval with well-defined margins and lack prominent peripheral echoes. • The lesions are primarily hypoechoic.
Imaging Studies: • CT scan is sensitive (88-95%), but the findings are not specific. • None of the imaging tests can definitely differentiate a • pyogenic liver abscess, an amebic abscess, or malignant disease. • Clinical, epidemiological, and serological correlation is needed for diagnosis








![[EPUB] DOWNLOAD Natural Liver Cleanse Recipes: Liver cleanse juices, liver cleanse tea, Liver cleanse soup, fatty liver](https://cdn7.slideserve.com/12507667/slide1-dt.jpg)