Download
1 / 41
410 likes | 808 Vues
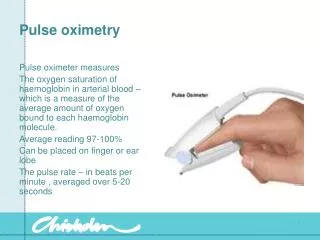
Unit 3.1 case studies PEFR and Pulse oximetry. By Elizabeth Kelley Buzbee AAS, RRT-NPS, RCP. Your patient is Mr. Rogers who presents in the ER with shortness of breath. To assess him further, you recommend:. answer. Getting a pulse oximetry reading to assess his level of hypoxemia

E N D
Unit 3.1 case studiesPEFR and Pulse oximetry By Elizabeth Kelley Buzbee AAS, RRT-NPS, RCP
Your patient is Mr. Rogers who presents in the ER with shortness of breath. To assess him further, you recommend:
answer • Getting a pulse oximetry reading to assess his level of hypoxemia • Listening to breath sounds to assess the presence and degree of bronchospasm • Inspecting him for use of accessory muscles, for his vital signs • Interviewing him for s/s of confusion or LOC
Mr. Rogers pulse oximetry reading is Sp02 88%. His respiratory rate 28 bpm and his heart rate is 119 bpm. • You:
answer • Suggest we start him on 1 lpm nasal cannula and repeat the pulse oximetry reading
answer • Repeat the pulse oximetry and reassess the vital signs. Both heart rate and respiratory rates should slow down a bit • look at his work of breathing and listen to his breath sounds to assess his respiratory distress
The doctor orders 2 lpm nasal cannula and you see that the heart rate and the respiratory rate are both decreased a bit. In 5 minutes, you see that the Sp02 rises from 88% to 90%. • Has the pulse oximetry been justified?
answer • Yes, • the patient has s/s of hypoxemia which you have monitored and documented with the pulse oximeter • You have successfully assess the effectiveness of the supplementary 02 by use of serial pulse oximetry readings
answer • While you reassessed the vital signs, you also need to assess the breath sounds which might tell us why the patient is hypoxic
On auscultation, you hear diffuse inspiratory and expiratory wheezes to all lobes. • You hear a prolonged expiratory time • What do you suggest now?
answer • Measure a PEFR to document the bronchospasm
The patient tries to follow your directions but coughs so much that she must stop. You suggest?
answer • Give the inhaled bronchodilator drugs and try to get the PEFR post bronchodilator
Case study # 2 • Your patient is Mr. Croder who has a history of COPD. • You would like to assess the following?
answer • Vitals signs • Interview the patient for his chief complaint: why is he in the hospital? • Inspection for s/s of shortness of breath • Breath sounds to assess the level of bronchospasm • Pulse oximetry if s/s of SOB
he in the hospital to have cardiac surgery • He is using accessory muscles to breath and is retracting • His breath sounds are diminished and there is scattered wheezing • Pulse oximetry shows 89% on room air • What do you suggest?
answer • Start him on supplementary 02 by 1-2 lpm nasal cannula • Reassess with a pulse oximetry • Assess his bronchospasm before and after a bronchodilator with a peak flow meter
The doctor orders a PEFR before and after administration of .5 mg Albuterol [a bronchodilator] • You need the following information to do this PEFR?
answer • From his chart get his age, height and sex • On the PEFR, look up the patient’s predicted PEFR based on this data
How do you explain the use of the Peak flow meter to the patient?
answer • Tell him to: • Put his lips and teeth on the mouth piece • Exhale as fast as he can into the meter • Read the meter • Repeat steps 1-3 until you get 2 readings that are within 5% of each other
answer • For reproducibility, you must have two readings that are close together • PEFR readings are patient-dependent and patient effort can drastically alter the reading so if you get two reading within 5% of each other, you can trust the data
The patient follows your directions but there is no reading on the peak flow meter. What has happened?
answer • Place nose clips on the patient to make sure he is exhaling through the peak flow meter • Double check that he has his lips tight around the mouth piece and that his teeth aren’t in the way • Make sure the one-way valve is pointed toward the meter
You see that the peak flow meter is not attached to the mouthpiece tightly so you tighten the connection and repeat the instructions. You get the following results: • 385 • 388 • 400 • Which of these PEFR measurements do you record?
answer • 400 lpm. It is the highest one and is within 5% of the next lowest
On the peak flow meter instructions, you see that this patient’s predicted PEFR is 645 lpm. • What is his % predicted?
answer • 400/645 = 62% • His PEFR is 62% of predicted
You give the .5 mg of Albuterol and reassess the patient. His respiratory rate is decreased and his retractions are decreased. On auscultation, you hear the scattered wheezing has decreased, but there are diminished breath sounds. When you repeat the PEFR you are not surprised to see the following
answer • The PEFR is now 445 lpm • If you calculate the % of predicted, you will discover that it has risen from 62% to 69% of predicted • 445 / 645 = 69% of predicted
Case study # 3 • Your patient Miss Otis, is a 25 year old who has been admitted to the ER secondary to injuries sustained during a fire. • What do you assess?
answer • Her state of consciousness is critical. If she is altered she may be in significant hypoxemia. • Her work of breathing is important. She may have upper airway swelling or bronchospasm • Auscultation of the chest for wheezing • Her PEFR might demonstrate the presence of significant bronchospasm
The patient is alert and anxious. She is using accessory muscles to breath and you hear wheezing bilaterally. • The nurse suggests we place a pulse oximeter on her finger. • You:
answer • Disagree, and recommend drawing blood for a co-oximetry reading. The Sp02 reading will be off.
answer • The presence of HbCO [carbon monoxide] in the blood would rise the color of the blood and fool the pulse oximeter which uses only two lights. You need all five lights of the co-oximeter to be sure of the presence of carbon monoxide
The doctor orders supplementary 02 by non-rebreathing mask and you see that the patient’s respiratory rate decreases, and her heart rate decreases after she is placed on extra 02. • What do you want to do for her?
answer • Assess her PEFR to document the presence of wheezing