Download
1 / 99
1.03k likes | 1.41k Vues
Amino Acids Dietary proteins are the primary source of a.a.s for endogenous protein synthesis.

E N D
Amino Acids • Dietary proteins are the primary source of a.a.s for endogenous protein synthesis. • - a.a.s in blood are filtered through the glomerular membranes then reabsorbed in the renal tubules by saturable transport systems. When the transport mechanism becomes saturated or is defective, a.a.s spill into the urine resulting in aminoaciduria. • Two types of aminoaciduria have been identified: • 1. Overflow aminoaciduria: which occurs when the plasma level of one or more a.a.s exceeds that of renal threshold (tubular capacity for reabsorption). • 2. Renal aminoaciduria: which occurs when plasma levels are normal but the renal transport system has a congenital or acquired defect.
The aminoaciduria - Aminoaciduria may be primary or secondary. Primary disease: due to an inherited enzyme defect, also called inborn error of metabolism. -The defect is located either in the pathway by which a specific a.a. is metabolized or in the specific renal tubular transport system by which the a.a. is reabsorbed. -The defect in the enzyme results in substrate accumulation or its diversion into alternative paths. Products of the normal path are not formed at all or formed in smaller amounts.
Secondary aminoaciduria: - Secondary aminoaciduria: could be due to either to disease of an organ such as the liver, which is an active site of a.a. metabolism, or a generalized renal tubular dysfunction. - It can affect many a.a. simultaneously Examples of disorders that result in secondary overflow amnioaciduria are acute viral hepatitis and acetaminophen poisoning. Generalized secondary renal aminoaciduria is due to progressive damage to the renal tubules It can be caused by poisons (especially heavy metal), or disease, or by congenital conditions such as Wilson’s disease.
Amino acid disorders • Phenylketonuria (PKU) • Urea cycle disorders • Tyrosinaemia type 1 • Homocystinuria • Maple syrup urine disease (MSUD) • Renal transport disorders • Cystinuria
Selected disorders of a.a. metabolism Hyperphenylalaninemias: these are a group of disorders resulting from impaired conversion of phenylalanine to tyrosine due to the defect in phenyalanine hydroxylase that found only in the liver and kidneys. Defects in this enzyme Hyperphenylalaninemia phenylalanine accumulates in blood, urine and CSF phenylketonuria (PKU) Untreated PKU results in severe mental retardation. * Affected children appear normal at birth, and the earliest symptoms are usually nonspecific-delayed development, feeding difficulties and vomiting. * Children with PKU elicit an unusual but characteristic musty odor in urine or sweat, owing to increased production of phenylpyruvate. * Early diagnosis is essential to avoid the adverse effects of PKU and consequently neonatal screening has become widespread.
Phenylketonuria (PKU) Elevated blood-phenylalanine activates the normal minor metabolic pathways of phenylalanine increased production of phenylketones (e.g., phenylpyruvate) and other metabolites that excreted into the urine. Treatment of PKU consists of restricting dietary phenyalanine before the onset of brain damage
Tyrosinemia * Tyrosinemia has several forms, each of which is accompanied by high level of tyrosine and phenolic aciduria. * Tyrosine is essential for protein synthesis and serves as a precursor for thyroxine, melanin and catecholamines. * The pigment melanin is derived from tyrosine by the activity of tyrosinase. * Clinical syndromes resulting from inherited defects in melanin synthesis are collectively known as albinism.
Cystinuria: • Classic cystinuria is the most frequently inborn error of a.a. transport. This disease is characterized by massive excretion of cystine, lysine, arginine and ornithine. • Normally these a.a.s are filtered by the glomerulus and reabsorbed in the proximal renal tubule. • In cystinuria re-absorption fails because a carrier system that transports all a.a.s is defective. • Because cystine is the least soluble of all the naturally occurring a.a.s, its overexertion often leads to the formation of cystine caliculi in the renal pelvis, ureters, and bladder; obstruction, infection, and renal insufficiency occasionally result. • Treatment involves reducing the concentration of cystine in urine by drinking large amounts of water, increasing cystine solubility by maintaining the urine alkaline and, if necessary, reducing cystine excretion by using pencillamine
Maple syrup urine disease: • Maple syrup urine disease (MSUD) takes its name from the characteristic maple syrup or burnt sugar odour of the urine of affected persons which is due to high concentrations of aliphatic keto acids. • a.a. analysis of blood and urine show high levels of leucine, isoleucine and valine. • These branched-chain a.a.s are normally converted by transamination to their corresponding -keto acids, by the enzyme branched-chain amino transfersae then oxidized into acyl-coenzyme A (CoA) derivatives by branched-chain -keto acid dehydroghenase • An inherited defect in the enzyme branched-chain -keto acid dehydroghenase results in accumulation of the branched-chain a.a.s and their corresponding -keto acids in blood, urine and CSF.
PLASMA ENZYMES • Measurements of the activity of enzymes in plasma are of value in the diagnosis and management of a wide variety of diseases. • Most enzymes measured in plasma are primarily intracellular, being released into the blood when there is damage to cell membranes, • Small amounts of intracellular enzymes are present in the blood as a result of normal cell turnover. • When damage to cells occurs, increased amounts of enzymes will be released and their concentrations in the blood will rise. • However, such increases are not always due to tissue damage. • Other possible causes include: increased cell turnover, cellular proliferation (e.g. neoplasia), increased enzyme synthesis (enzyme induction), obstruction to secretion, decreased clearance. • Many other enzymes, for example renin, complement factors and coagulation factors, are actively secreted into the blood, where they fulfill their physiological function.
A major disadvantage in the use of enzymes for the diagnosis of tissue damage is their lack of specificity to a particular tissue or cell type. Many of these enzyme are not used as diagnostic tool but used for monitoring the diseases Many enzymes are common to more than one tissue This problem may be overcome to some extent in two ways: A) First, different tissues may contain (and thus release when they are damaged) two or more enzymes in different proportions; e.g. alanine and aspartate aminotransferase are both present in cardiac muscle and hepatocytes, but there is relatively more alanine transaminase in the liver; B) Second, some enzymes exist in different forms (isoforms), termed isoenzymes. Individual isoforms are often characteristic of a particular tissue. So the pattern of increase of different enzymes can indicate the site of problem, e.g. high GGT and high ALP or AST indicates a problem in the liver While high ALT and CK-MB indicates MI
Factors Affecting Results of Plasma Enzyme Assays Analytical factors affecting results. Results of enzyme assays are not usually expressed as concentrations, but as activities. So the results of such measurements depend on many analytical factors including the concentrations of the substrate and product, the pH and temperature at which the reaction is carried out, the type of buffer, and the presence of activators or inhibitors. Physiological factors affecting enzyme activities, include for example: age: plasma aspartate transaminase activity is moderately higher during the neonatal period than in adults; plasma alkaline phosphatase activity of bony origin is higher in children than in adults. sex: plasma gama-glutamyltransferase activity is higher in men than in women physiological conditions: plasma alkaline phosphatase activity rises during the last trimester d pregnancy because of the presence of the placental isoenzyme; several enzymes, such as the transaminases and creatine kinase, rise moderately in plasma during and immediately after labour or strenuous exercise.
Two important transferases: Alanine aminotransferas (ALT) called also Glutamate – Pyruvate transferase (GPT) or Serum ALT = SGPT, found in many tissues catalyzes the transfer of amino gp of alanine to produce pyruvate and glutamate. Aspartate aminotransferase (AST) called also Glutamate–Oxaloacetate transferase (GOT) or Serum AST = SGOT, - During the catabolism of amino acids AST takes amino group from glutamate to oxaloacetate forming aspartate. Which used as source of NH4 group in Urea synthesis Aspartate source of amino group of the urea in the urea cycle.
Aspartate Transaminase (AST): 10-45 U/L AST (glutamate oxaloacetate transaminase GOT) is present in high concentrations in cells of cardiac and skeletal muscle, liver, kidney and erythrocytes. Damage to any of these tissues may increase plasma AST levels. AST can be used as indicator of muscle damage. Causes of Raised Plasma AST Activities * Artifact: due to in-vitro release from erythrocytes if there is haemolysis or if separation of plasma from cells is delayed. *Physiological: during the neonatal period (about 1.5 times the upper adult reference limit). *Marked increase (10 to 100 times the upper adult reference limit): circulatory failure with 'shock' and hypoxia; myocardial infarction; acute viral or toxic hepatitis.
Aspartate Transaminase (AST) *Moderate increase: Cirrhosis (may be normal, but may rise to twice the upper adult reference limit); infectious mononucleosis (due to liver involvement (type of viral infection “mononucleosis” refers to an increase in a special type of white blood cells (lymphocytes); cholestatic jaundice (up to 10 times the upper adult reference limit); malignant infiltration of the liver; skeletal muscle disease; after trauma or surgery (especially after cardiac surgery); severe hemolytic episodes (of erythrocyte origin).
Alanin Transaminase (ALT): 10-50 U/L • ALT (glutamate pyruvate transaminase, GPT) is present in high concentrations in liver and, to a lesser extent, in skeletal muscle, kidney and heart • ALT is more specific for liver than muscle • Causes of Raised Plasma ALT Activities • *Marked increase (10 to 100 times the upper limit of normal (ULN)): • - acute viral or toxic hepatitis. • - circulatory failure with 'shock' and hypoxia; • *Moderate increase: • -cirrhosis (may be normal or up to twice*ULN); • -infectious mononucleosis (due to liver involvement); • -liver congestion secondary to congestive cardiac failure; • -cholestatic jaundice (up to 10 times the upper reference limit in adults); • -surgery or extensive trauma and skeletal muscle disease (much less affected than AST).
Gamma-glutamyl-transferase (GGT) • GGT occurs mainly in the cells of liver, kidneys, pancreas and prostate. • Plasma GGT activity is higher men <50 U/L) than in women <30 U/L. • It is very sensitive but unspecific indicator for liver dysfunction; • Sensitive anything wrong in the liver will elevate its activity but non-specific can’t indicate the reason of liver disease • Causes of raised plasma GGT activity • -Induction of enzyme synthesis, without cell damage, by drugs or alcohol. Many drugs most commonly the anticonvulsant phenobarbitone and phenytoin, and alcohol induce proliferation of the endoplasmic reticulum. • Cholestatic liver disease, (cholestasis is a condition where bile cannot flow from the liver to the duodenum): changes in GGT activity usually parallel those of alkaline phosphatase. • In biliary obstruction, plasma GGT activity may increase before that of alkaline phosphatase. • Hepatocellular damage, such as that due to infectious hepatitis; measurement a plasma transaminase activities is a more sensitive indicator of such conditions. • Plasma GGT activity is frequently very high in patients with alcoholic liver disease and can be elevated, due to enzyme induction, the absence of of liver damage
Alkaline Phosphatase (ALP) -The alkaline phosphatases are a group of enzymes that hydrolyze organic phosphates at high pH. -They are present in most tissues but are in particularly high concentration in the osteoblasts of boneand the cells of the hepatobiliary tract, intestinal wall, renal tubules and placenta. -The exact metabolic function of ALP is unknown but it is probably important for calcification of bone. - In adults plasma ALP is derived mainly from bone and liver in approximately equal proportions; the proportion due to the bone fraction is increased when there is increased osteoblastic activity that may be physiological.
Causes of raised plasma ALP activity Physiological: during the last trimester of pregnancy the plasma total ALP activity rises due to the contribution of the placental isoenzyme Bone disease: Rickets and osteomalacia; Rickets: is an abnormal bone formation in children resulting from inadequate calcium in their bones Osteomalacia: softening of the bones, resulting from defective bone mineralization in adults Paget's disease and (ALP may be very high); Paget's disease is a chronic bone disorder that is due to irregular breakdown and formation of bone tissue. Primary hyperparathyroidism with extensive bone disease Liver disease: intra- or extrahepatic cholestasis, lesions, tumor, granulomas, and other causes of hepatic infiltration. Malignancy: bone or liver involvement or direct tumor production.
Lactate dehydrogenase Homolactic fermentation: conversion of pyruvate to lactate • Reduction of pyruvate to lactate • Lactate is formed by the action of Lactate dehydrogenase • It is the final product of anaerobic glycolysis in eukaryotic cells • It is also formed in RBC, lens and cornea of the eye, kidney medulla, testes and leukocytes
Lactate Dehydrogenase (LD): 110-230 U/L • - The enzyme is widely distributed in the body, with high concentrations in cells of cardiac and skeletal muscle, liver, kidney, brain and erythrocytes; • Measurement of plasma total LD activity is therefore a nonspecific marker of cell damage. • Causes of Raised Plasma Total LD Activity. • Artifact: • due to in vitro haemolysis or delayed separation of plasma from whole blood. • Marked increase (more than 5 times ULN): • -Circulatory failure with 'shock' and hypoxia; • - Myocardial infarction • Some hematological disordersas megaloblastic anaemia, acute leukaemias and lymphomas,
Creatine Kinase (CK) CK is most abundant in cells of cardiac and skeletal muscle and in brain, but also occurs in other tissues such as smooth muscle. Causes of raised plasma CK activities *Artifact: due to in vitro haemolysis *Physiological: neonatal period (slightly raised above the adult reference range). Marked increase: Circulatory failure and shock; myocardial infarction; Muscular dystrophies and high breakdown of skeletal muscle. The muscular dystrophies are the most-known group of hereditary muscle diseases; characterized by progressive skeletal muscle weakness, defects in muscle proteins, and the death of muscle cells and tissue.
Creatine Kinase (CK) Moderate increase: Muscle injury; after surgery (for about a week); physical effort, moderate exercise and muscle cramp; an intramuscular injection; hypothyroidism (thyroxine may influence the catabolism of the enzyme); alcoholism (due to alcoholic myositis (inflammation of the muscle) ISOENZYMES OF CK CK has 3 isoenzymes: CK-MM (CK-3) is the predominant isoenzyme in skeletal and cardiac muscle and is detectable in the plasma of normal subjects. CK-MB(CK-2) accounts for about 35 % the total CK activity in cardiac muscle and less than 5% in skeletal muscle; Its plasma activity is always high after myocardial infarction. CK-BB (CK-1) is present in high concentrations in the brain and in the smooth muscle of the gastrointestinal and genital tracts. Raised plasma activities may occur during labour and child birth.
Non-specific Causes of Raised Plasma Enzyme Activities Change in plasma enzyme activity could be due to nonspecific causes -Slight rises in plasma aspartate transaminase activities are common in non-specific findings in many illnesses. - Moderate exercise, or a large intramuscular injection, may lead to a rise in plasma creatine kinase activity; - Some drugs, such as the anticonvulsants phenytoin and phenobarbitone, may induce synthesis of the microsomal enzyme, gammaglutamyltransferase, and so increase its plasma activity in the absence of disease. - Plasma enzyme activities may be raised if the rate of clearance from the circulation is reduced.
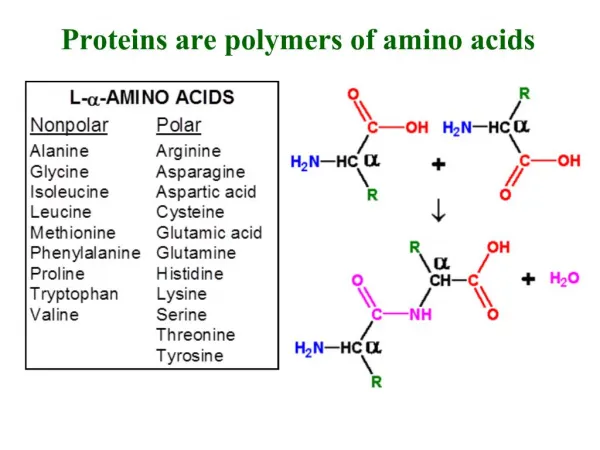
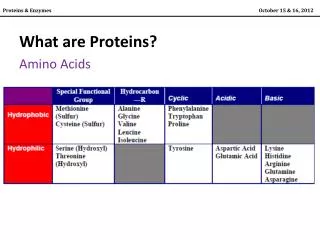
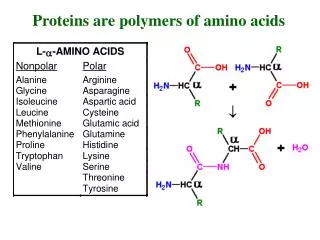
Plasma Proteins Proteins: are polymers of a.a.s that are covalently linked through peptide bonds. The different R groups found in a.a.s influence the structure, functionality and properties of the individual proteins. Proteins may be classified as fibrous (mainly structural) or globular. *Nearly all other proteins of clinical interest are soluble globular proteins such as haemoglobin, enzymes and plasma proteins. *The complex bending and folding of polypeptide chains is a result of numerous interactions of their R groups. *Globular proteins are compact and have little or no space of water in the interior of the molecule, where most of the hydrophobic R groups are located. *Most polar R groups are located on the surface of the protein where influence on protein solubility, acid-base behaviour and electrophoretic mobility *Most globular proteins are affected with temperature and pH.
Plasma proteins • Over 100 individual proteins have a physiological function in the plasma. Quantitatively, the single most important protein is albumin. The other proteins are known collectively as globulins.
Protein Properties - Many of the properties of proteins are used for their separation, identification and assay: 1-Molecular size: Most proteins are macromolecules, so can be separated from smaller molecules by dialysis or ultrafiltration, chromatography and by density-gradient ultracentrifugation 2. Differential solubility: Protein solubility is affected by the pH, ionic strength, temperature and dielectric constant of the solvent. 3. Electrical charge: Separation by electrophoresis, this is based on the capability of a mixture of proteins with various species of different charge/mass ratiosto migrate at different rates in an electrical field. 4.Adsorption on finely divided inert materials: These materials offer a large surface area for interaction with protein, such as charcoal, silica or alumina. 5. Specific binding to antibodies, coenzymes, or hormone receptors: The unique properties of protein to recognize and bind to a complementary compound with high specificity is the basis for immunoassays.
Analysis of proteins • Methods for the analysis of proteins in body fluids can be grouped as follows: • Quantitative measurements of total protein and albumin. • Separation by electrophoresis, which provides semiquantitative estimations of the main classes of proteins present in fairly high concentrations. • Specific quantitative assays of particular proteins by immunoassays using specific antisera and measurement of antigen-antibody complexes. • Detection and identification of abnormal proteins.
Serum Protein Electrophoresis *Electrophoresis separates proteins according to their different electrical charges *It is usually performed by applying a small amount of serum to a strip of cellulose acetate or agarose and passing a current across it for standard time.
Serum Protein Electrophoresis Electrophoresis separates proteins into five main groups of proteins, albumin and the 1-,2-,- and -globulins, Anode Cathode Anode Cathode
Principal bands seen after electrophoresis on cellulose acetate of normal adult serum 1. Albumin, usually a single protein, makes up the most obvious band. 2. 1-Globulins consists almost entirely of 1-antitrypsin. 3. 2-Globulins consists mainly of 2-macro-globulin and haptoglobin. 4. -Globulins often separate into two; 1 consists mainly of transferrin with a contribution from LDL and 2 consists of C3 complement. 5. -Globulins are immunoglobulins. Some immunoglobulins are found also in the 2 and regions. - If plasma rather than serum is used, fibrinogen appears as a distinct band in the - region. This may make interpretation difficult; blood should be allowed to clot and serum used if electrophoresis is to be performed.
Many other important proteins are present in only very low concentration
Serum protein electrophoresis: applied to the serum not plasma *Electrophoresis separates proteins into five main groups of proteins, albumin and the 1-,2-,- and -globulins, may be distinguished after staining and may be visually compared with those in a normal control serum. *Each of the globulin fractions contain several proteins. *Changes in electrophoretic patterns are most obvious when: 1. The concentrations of protein, such as albumin, which is usually in high concentration, are abnormal. 2. There are parallel changes in several proteins in the same fraction. 3. New band that is not seen in normal serum.
Electrophoretic patterns in disease: • Some abnormal electrophoretic patterns are characteristic of a particular disorder or while others indicate non-specific pathological processes. • For example, the 2 band which contains haptoglobin may be reduced if there is in vivo haemolysis and split into two if in vitro haemolysis has occurred. • Parallel changes in all fractions. Reduction may occur in sever malnutrition, unless accompanied by infection or haemodilution. • The acute-phase pattern. Tissue damage of any kind triggers the sequence of biochemical and cellular events associated with inflammation. The biochemical changes include stimulation of synthesis of the so-called acute-phase proteins, with a rise in the 1- and 2-globulin fractions increase the erythrocyte sedimentation rate (ESR). • Chronic inflammatory state: usual increase in immunoglobulin synthesis may be visible as a diffuse rise in -globulin. • Nephrotic syndrome. Plasma protein changes depend on the severity of the renal lesion.
Plasma proteins • Proteins are present in all body fluids including blood plasma. These proteins are examined frequently for diagnostic purposes. • The amount of protein in the vascular compartment depends on the balance among: • The rate of synthesis • The rate of catabolism or loss • The relative distribution between the intra- and extravascular compartments the concentration depends on the relative amounts of protein and water in the vascular compartment. • Many plasma proteins are synthesized in the liver. Some proteins are synthesized both in cells and macrophages. Immunoglobulins are mainly derived from the B cells of the immune system. • Most plasma proteins are taken up by pinocytosis into the capillary endothelial cells or mononuclear phagocytes where they are catabolized. Some are catabolized by renal tubular cells. • Small proteins are lost passively through the renal glomeruli and intestinal wall. Some are reabsorbed, either directly by renal tubular cells or after digestion in the intestinal lumen
Total plasma protein (62-80 gm/L) - Alterations in plasma protein can be due to A) Change in the concentration of a specific protein in plasma (due to changes in the rate of synthesis or removal) B) Change in the volume of distribution (plasma water). *Decrease in the volume of plasma water (haemoconcentration) as relative hyperproteinaemia concentrations of all plasma proteins are increased to the same degree *Hyperproteinaemia is caused by: 1) dehydration (haemoconcentration) due to inadequate water intake or excessive water loss, as in sever vomiting, diarrhoea, diabetic acidosis. 2) an increase in the concentration of specific protein normally present in relatively low concentration, as, for example, increases in APRs and polyclonal or monoclonal immunoglobulins as a result of infection. *Hypoproteinaemia: caused by a) decreased synthesis, b) Haemodilution and c) protein redistribution. Haemodilution (increase in plasma water volume) hypoproteinaemia; concentrations of all the individual plasma proteins are decreased to the same degree. Haemodilution occurs with water intoxication or salt retention syndromes, during massive intravenous infusions.
Total plasma protein • *A rapid decrease in protein concentration is most frequently due to • 1) An increase in plasma volume. • 2) Capillary permeability increases in patients with septicaemia or generalised inflammatory conditions since proteins will diffuse out into the interstitial space. • * The concentration of plasma proteins is affected by posture • * Albumin is present in such high concentrations that low levels of this protein alone may cause hypoproteinaemia • *Plasma total proteinconcentrations may be misleading: They may be normal in the presence of quite marked changes in the constituent proteins. • a fall in plasma albumin concentration may be balanced by a rise in immunoglobulin concentrations, it is quite common. • Most individual proteins except albumin contribute little to the total protein concentration; quite a large percentage change in the concentration of one may not cause a detectable change in the total protein concentration.
Plasma protein can be divided into 1) Acute phase reactants (APR) these proteins have specific role in inflammatory response so they will increase in inflammatory conditions 2) Negative acute phase reactants these proteins have no role in in inflammation but number of these proteins decrease in inflammatory conditions. Like albumin, prealbumin, transferrin ….
Specific plasma proteins • Albumin (35-47 gm/L) • * The most abundant plasma protein representing 40-60% of the total protein. • * It is synthesised in the liver at a rate that is dependent on protein intake but subject to feedback regulation by the plasma albumin level. • * Contributes largely to the oncotic pressure of plasma. Oncotic pressure is the osmotic pressure due to the presence of proteins and is an important determinant of the distribution of extracellular fluid (ECF) between the intravascular and extravascular compartments. • * The chief biological functions of albumin are to: • Transport and store wide variety of ligands. • Maintain the plasma oncotic pressure. • Serve as a source of endogenous a.a.s.
Hypoalbuminaemia * Low albumin concentration may be due to dilution or redistribution. * True albumin deficiency may be caused by a decreased rate of synthesis, or by an increased rate of catabolism or loss from the body.
Consequences of hypoalbuminaemia 1. Fluid distribution. The decreased plasma oncotic pressure disturbs the equilibrium between plasma and interstitial fluid there will be a decrease in the movement of the interstitial fluids back into the blood accumulation of interstitial fluid (edema) relative decrease in plasma volume fall in renal blood flow stimulates the secretion of renin, and aldosterone through the formation of angiotensin sodium retention and thus an increase in ECF volume which potentiates the edema. 2. Binding functions. Albumin is a high capacity, low affinity transport protein for many substances, such as thyroid hormones, calcium, bilirubin and fatty acids. Many drugs are bound to albumin in the blood stream as salicylates, penicillin and sulphonamides. The drug fraction that is bound to albumin is physiologically and pharmacologically inactive A reduction in plasma albumin, may increase the plasma free concentration of those drugs cause toxic effects
Hyperalbuminaemia • Hyperalbuminaemia may be due to : • An artefact, a result of venous stasis during blood collection (a sample that was taken from an arm at an excessively long cuffing period) • Over-infusion of albumin • Dehydration: high level of plasma albumin-greater than 50 g/l is usually indicative of severe dehydration. • Albumin synthesis is increased in some pathological states but never causes hyperalbuminaemia. • The plasma albumin concentration is used as a test of liver function. Because of its relatively long half-life (approximately 20 days) in the plasma, • Albumin concentration is usually normal in acute hepatitis. • Albumin test isnot useful marker for short term acute function of the liver • Low Albumin concentrations are characteristic of chronic liver disease, due to both decreased synthesis and an increase in the volume of distribution as a result of fluid retention and the formation of ascites (free fluid in the peritoneal cavity).
2-Macroglobulin (α2M) • The largest plasma protein. • 2-Macroglobulin inhibits proteases that released in inflammatory conditions and destroy the tissues and cells its main function to protect tissues from proteases and it is not released during acute inflammation. • It is not APR. • Because of its large size, it tends to remain in the intravascular compartment. • It is synthesised in the liver and in the reticuloendothelial system. • It increases in nephrotic syndrome, because it is retained and will not be lost because of its large size. • Its hepatic synthesis increases in order to compensate partially for the decrease in albumin normally active in maintaining the oncotic pressure.
Transferrin (TRF) : B-globulin protein (2.1-3.6 g/L) • * It is synthesized mainly in the liver, and in the endocrine glands as ovaries and tests. * TRF is a -globulin which is the major iron-transporting protein in the plasma. * It reversibly binds numerous cations iron, copper, zinc, cobalt and calcium-although only iron binding appear to have physiological significance. * TRF is normally about 30-40% saturated with iron and its half life 7 days. * Its concentration correlates with the total iron-binding capacity of serum. • Measurements of plasma transferrin level is useful for the differential diagnosis of anaemia and for monitoring its treatment.
Transferrin (TRF) : (2.1-3.6 g/L) *TRF Plasma levels are regulated by availability of iron iron deficiency, TRF rise and, upon successful treatment with iron, it returns to normal level. * In common iron deficiency, the TRF level is increased due to increases in synthesis this guarantee that any amount of iron absorbed will be transported and bound to TRF directly and in this case the % of saturation will be less than 30% the protein is less saturated with iron because plasma iron levels are low *If the anemia is due to failure to incorporate iron into erythrocytes, Vit B12 or folic acid deficiency the TFR level is normal or low but the protein is highly saturated with iron. High levels of TRF occur in pregnancy and oestrogen administration.
1-Fetoprotein (AFP) • - It is the principal foetal protein. • - Appears in infantile urine it presents in amniotic fluid and maternal blood • It is determined in amniotic fluid and in maternal serum for the antenatal diagnosis (tests before the birth) of neural tube defects. • Neural tube defect (NTD): A major birth defect caused by abnormal development of the neural tube, the structure present during embryonic life which gives rise to the central nervous system ‘the brain and spinal cord”. Neural tube defects (NTDs) are among the most common birth defects that cause infant mortality (death) and serious disability. There are a number of different types of NTDs • During the foetus growth the CNS starts with the spinal cord then the nervous system 1-Fetoprotein test is done in the 4th months of pregnancy to make sure that CNS of the foetus is developing normally. High level of this protein due theleakage to the amniotic fluid and to mother serum indicates defect in CNS development • - Detection of higher AFP than the normal in early pregnancy can suggest CNS defects • * Gross elevations of AFP serum levels are found in approximately 80% of patients with hepatocellular carcinoma, • * Sequential assays are particularly useful for prognosis and for monitoring treatment.