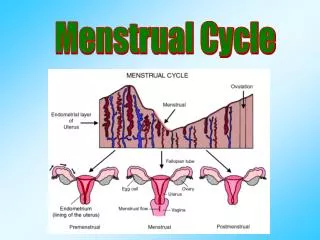
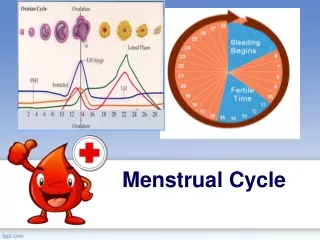
Menstrual Cycle
The Menstrual Cycle is a natural, recurring process that prepares the female body for potential pregnancy. Typically spanning 21 to 35 days, it involves a complex interplay of hormones that regulate changes in the ovaries and uterus. Understanding this cycle is crucial for reproductive health, fertility awareness, and overall well-being


Menstrual Cycle
E N D
Presentation Transcript
Dr. Sagar D. Dherange MS OBGYN-A Menstrual cycle
It is the visible manifestation of Cyclic, Physiologic, Uterine Bleeding due to shedding of endometrium menstruation
Composition Dark colored flow containing Blood, Mucus, Vaginal Epithelium Cell, Fragment Of Endometrium, Prostaglandin, Enzyme, Bacteria Physiology of menstruation
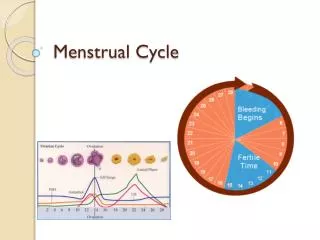
Menarche 11-15 yrs (Avg 13 yr) Interval 21-35 days (Avg 28 days) Duration 4-5 days Blood loss 20-80 ml (Avg 35 ml) Menopause 45-50 yrs Physiology of menstruation
Origin - endoderm of yolk sac in hindgut No. At 20 wk(intra uterine) 6-7 million At birth 2 million At puberty 4,00,000 In entire life 400 Tendency of sex cell to undergo degeneration which starts in intrauterine life upto menopause Germ cell
Upto Puberty Mitosis After Puberty Prophase of Meiosis After Puberty Meiosis 1 After Fertilization Meiosis 2 Cell division
Arrested meiotic division of oocyte prior to ovulation is probably due to oocyte maturation inhibition (OMI) factor present in follicular fluid secreted by granulosa cells gametogenesis
It include • Development & maturation of follicles • Recruitment of group of follicles • Selection of dominant follicles • Ovulation • Formation of corpus luteum • Degeneration of corpus luteum Ovarion cycle
The process takes 85 days & spreads over 3 ovarian cycles • About 20 antral follicles processed to develop in each cycle • Initially not under any hormonal control after 2-5 mm size growth controlled by FSH • Without FSH they undergo atresia Recruitment of group of follicles(Pre antral phase)
At day 5-7 the follicle which having • Highest antraloestrogen • lowest antral androgen • Whose granulosa contain maximum receptor for FSH Is selected & rest become atretic by day 8 Selection of dominant follicle
LH Surge (24 hrs) • Completion of reduction division of oocyte • Luteinization of follicle • Synthesis of progesterone & prostaglandin FSH Rise • Increased plasminogen • increased plasmin • increased lysis of wall of follicle Stretching factor • (increased intra follicular fluid 10-15 mmhg) Contraction of micro muscles • (local PG synthesis) ovulation
Causes Oogonia not having granulosacelll envelop Follicle not going meiotic division/not rescued by FSH Not having/lost FSH receptor (loss due to increased androgen negative feeedback by dominant follicle) Genetic (45 xo) Apoptosis(programmed cell death) Action of androgen To enhance process of atresia To stimulate libido( in mid menstrual period) FOLLICUL;AR ATRESIA
Starts before menstruation stops & completede 2-3 days after end of menstruation • Surface epithelioum derived from lamina gland & stromal cells • New blood vessels grows, glands & stromal cell regenerate • Size 2mm regeneration
From 5th 6th day to 14th day(till ovulation) • Proliferation occurs due to estrogen • Gland become tubular & perpendicular • Epithelial become columnar & nuclei at base • Spindle shaped stromal cell with mitosis • Soiral vessels unbranched to a region below epithelium • Size 3-4 mm proliferation
Endometrium contain receptor for progesterone which induced by estrogen • Progesterone can only act on endometrium previously primed with estrogen • From day15 to 5-6 days prior to menstruation • Surface epithelium more columnar & ciliated • Gland increases in size • Lining epithelium become taller & vacuolation occur(progesterone effect) persist upto 21st day of cycle Secretory phase
Intracellular secretion enter gland lamina pushing nuclei back toward basement. Gland become cork screw shaped & blood vessels undergo spiralling • Stromal cells swollen, large, poly hedral deeper spongy layer contain convoluted gland,coiledsrterioles,fewstromal cell • By dehydration of gland ,growth ceases spiral vessels & capillaries engorged by withdrawl hormone the basal parts of arteries undergo intense spasm leading to stasis of tissue anoxemia (24-48hours prior to menstruation) Secretory phase
Proliferative secretory Histological changes in endometrium
Degeneration & casting off of endometrium prepared for pregnancy due to regression of corpus luteum with fall in level of estrogen & progesterone Menstrual phase
The menstrual Rhythm depends upon the Hypothalamo -Pituitary -Ovarian axis • The blood loss depends upon the condition of uterus. Endocrinology of menstrual cycle
H-P-O-U Axis GnRh FSH &LH Estrogen & Progesteron
Peptide hormone • Secreted by hypothalamus • Half life 2-4 minutes • Stimulates secretion of FSH & LH by pituitary • Released in Pulsatile fashion • Follicular phase Once in 60 minutes Low amplitude • Luteal phase once in 90-120 minutes High amplitude Gnrh
Granulosa Cell Theca Cell Avascular Vascular TWO CELL TWO GONADOTROPHIN THEORY LH FSH LDL Cholesterol Androgen Androgen Estrogen Aromatase
Glycoprotein • Stimulated by GnRh production • Suppressed by estrogen & inhibin • Two peaks levels during menstrual cycle • Follicular phase (6th day) • Pre ovulatory phase (12th day) • Functions • Recruitment of follicles • Follicular growth • Acts on granulosa cells Increase in number Increase in LH receptors Increase in aromatase activity FSH
Glycoprotein • Stimulated by GnRH and high level of oestrogen • Suppressed by moderate level of oestrogen • Present in low levels throughout menstrual cycle • Peak level 24–36 hours before ovulation • Functions • Triggers ovulation • Stimulates androgen production by theca cells • Stimulates synthesis of progesterone by corpus luteum LH
Steroid hormones • Oestradiol, oestrone and oestriol • Site of production • Ovary(Mainly oestradiol Small amount of oestrone) • Adipose tissue(Oestrone) • Foetal liver(Oestriol) • Synthesized by granulosa cells • Predominant hormone of follicular phase • Inhibit FSH • Trigger LH surge ESTROGEN
Steroid hormone • Site of production Ovary,Adrenal glands • Synthesized by theca cells • High levels in luteal phase • Low levels indicate anovulation • Prepares endometrium for implantation PROGESTERONE
Polypeptide hormone • Controls milk secretion by breast • Under inhibitory control of the hypothalamus • Inhibited by dopamine • Stimulated by • TRH • Vasopressin • Vasoactive intestinal peptides • Endogenous opioids PROLACTIN
FSH stimulate granulosa cell to secrete peptide Inhibin,Activin, Follistatin • Peptides • Produced by ovary • Have endocrine and paracrine functions OTHER PEPTIDE
Inhibin Two forms: A and B Inhibits FSH Stimulates ovarian androgen production • Activin Stimulates FSH release Aromatase activity Progesterone synthesis Inhibin,Activin
Follistatin Binds activin Inhibits FSH Accelerates oocyte maturation • FSH & LH action are modulated by IGF,EGF • IGF 11 stimulate Aromatase activity leading to increased progesterone Follistatin
PGF2a- Myometrial Contraction & Vasoconstriction PGE2- Myometrial Contraction & Vasodilatation PGI2- Myometrial Relaxation & Vasodilatation prostaglandin
THANK YOU JUST GO WITH THE FLOW