Download
1 / 73
840 likes | 1.42k Vues
Management of Renal Artery Stenosis. Kent MacKenzie, MD Division of Vascular Surgery McGill University Montreal, Quebec. Disclosures. None. Atherosclerotic RAS. Often orificial/ostial Associated aortic atherosclerosis Associated atherosclerosis elsewhere Coronary Carotid Peripheral

E N D
Management of Renal Artery Stenosis Kent MacKenzie, MD Division of Vascular Surgery McGill University Montreal, Quebec
Disclosures None
Atherosclerotic RAS • Often orificial/ostial • Associated aortic atherosclerosis • Associated atherosclerosis elsewhere • Coronary • Carotid • Peripheral • Fibrointimal Hyperplasia (FMD)
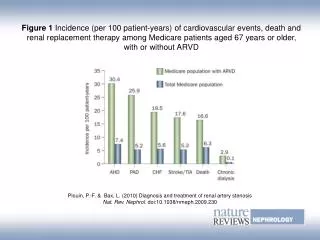
Atherosclerotic RAS • Clinical Consequences • Hypertension • Ischemic nephropathy • Chronic renal failure • Dialysis
Hypertension • Picture Renin-AII-Ald
Angiotensin II • Vasoconstriction • Sodium Retention • Aldosterone Release
Sustained HTN • Adaptive changes PVR • Heart • Arteries • Endothelial dysfunction • Nitrous oxide
The presence of hypertension is considered a prerequisite for renal artery intervention.
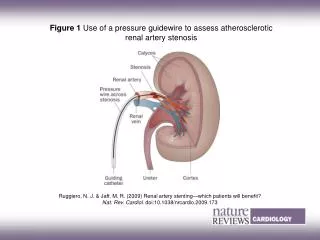
Diagnosis of RAS • Hemodynamically significant lesion in renal artery in a patient with HPTN • Pressure gradient • Diagnosis depends on identifying: • a pressure gradient • surrogate of a pressure gradient • Functional surrogate • Imaging surrogate
Functional Studies • Intravenous Pyelography • Differential Renal Function Studies • Plasma Renin Activity • Simulated Plasma Renin Activity • Renal Vein Renin • Catpopril Renal Scintography
Imaging Diagnosis • Imaging surrogates for hemodynamic RAS • Duplex ultrasound • CT • MRA • Angiography
CT Angio • Minimally invasive • Calcification artifact
MRA • NSF • ?overestimates • experience
Duplex Ultrasound • PSV criteria • PSV RA/Aorta ratios Picture
Angiography • ? Smaller contrast load • Allows intervention
In Practice • High likelihood of RAS • Good clinical indications for intervention • Duplex ultrasound • Ad-hoc Diagnostic +/- Therapeutic renal arteriography
Indications for Revascularization The presence of hypertension is considered a prerequisite for renal artery intervention.
Revascularization • Potential Indications for renal revascularization • Incidental , asymptomatic RAS with need for aortic reconstruction • RAS with renal dysfunction alone • RAS with hypertension • RAS with hyperpertension and renal dysfunction • RAS with angina • RAS with recurrent flash pulmonary edema Chronic HPTN issues Acute HPTN issues
Revascularization with aortic surgery (prophylactic) • 69 y.o. patient requires: • Open AAA repair • Endo AAA repair • Aortofemoral bypass for occlusive dx. • Incidental imaging finding of severe RAS • No severe HPTN at diagnosis
Revascularization with aortic surgery (prophylactic) • 100 hypothetical patients with unsuspected RAS who will undergo aortic surgery • 44% (44 patients) lesion progression and RVH • 36% (16 patients) may develop preventable reduction in renal function • 66% (11 patients) will demonstrate restored function with delayed renal treatment Hansen KJ et al
Revascularization with aortic surgery (prophylactic) • Therefore only 5 patients (5%) will gain a unique benefit from prophylactic renal artery repair • Risk of adverse event with combined aortic/renal revasc. • 5-6% mortality in the best hands • 3-4% late failure of operative repair • Therefore, prophylactic renal revasc. will potentially result in benefit in 5% of patients yet an adverse outcome in 10% Hansen KJ et al
Revascularization with aortic surgery (prophylactic) • Prophylactic renal revascularization alone or in conjunction with aortic reconstruction is therefore not indicated • Surgical reconstruction • Catheter-based reconstruction Hansen KJ et al
Renal Insufficiency and RAS • The absence of hypertension in a patient with RAS and excretory dysfunction suggests the presence of severe parenchymal disease • Without HPTN, response to revascularization is poor
RAS and Hypertension alone • Treatment is empiric • Expectation of clinical improvement is less • Unilateral vs. Bilateral RAS • Hypertension response is poorly predictable
Hypertension with Renal Insufficiency • Accumulated experience has resulted in a paradigm shift in approach to selecting patients for intervention • Surgical literature PTA • RAS and severe HPTN as a pre-intervention predictor of response • Changes in renal function post-intervention being the short-term outcome • Improvements in all-cause cardiovascular outcomes being the outcome of interest in trials evaluating RA intervention
Hypertension with Renal Insufficiency All patients
Hypertension with Renal Insufficiency • Treatment of hemodynamically significant RAS in a patient with: • Hypertension (severe) • Rapidly progressive decline in renal function • Salvageable renal mass • Surgical literature suggests expectation of improved BP control and reduction in rate of functional loss
RAS with angina or pulm edema • Acute myocardial strain • Acute episodes of severe hypertension • Multiple case-series suggesting significant stabilzation of cardiac status after renal revascularization
Options for Intervention • Surgical Revascularization • Renal/aortic endarterectomy • Renal artery bypass • Direct • Aortorenal bypass, iliorenal bypass • Renal artery reimplantation • Indirect • Hepatorenal bypass • Splenorenal bypass • Mesorenal bypass
Surgical Revascularization Ex-vivo reconstruction To be considered in: Solitary kidney Complex renal artery branch reconstructions Options for Intervention
Options for Intervention • Percutaneous Treatment • Renal artery angioplasty • Renal artery angioplasty with provisional/selective stenting • Renal artery stenting
No controlled studies comparing angioplasty vs. stenting • Limited data comparing angioplasty/stenting to surgical revascularization • No strong evidence demonstrating superiority of surgical revascularization over medical therapy • No strong evidence demonstrating superiority of renal angioplasty/stenting over medical therapy • Uncontrolled, non-randomized data supports the use of renal revascularization in high-risk groups
Side-by-side comparison of large surgical series and renal angioplasty series suggests better durability and improvements in renal insufficiency in surgical patients • Comes at the cost of higher peri-procedural morbidity and mortality • So percutaneous treatments selected in most patients other than those with need for aortic reconstruction or with contraindications for PTA
Randomized Trials Percutaneous Renal Artery Intervention
EMMA Trial, 1998 • Unilateral atherosclerotic RAS • Normal renal function • 59 patients randomized • Primary outcomes • Ambulatory blood pressure (ABP) • Secondary outcomes • Treatment score • Complications
No difference in ABP • But lower Treatment Score (fewer meds) in angioplasty group • Higher procedural complication in angioplasty group (26% vs. 8%) • Criticisms: • 1/3 eligible screened patients not enrolled because of patient or physician preference for angioplasty • Protocol called for antihypertensives in angioplasty group if BP control ‘not optimal’ • Study design biased to not demonstrate primary outcome
Scottish/Newcastle study, 1998 • Atherosclerotic uni- or bilat- RAS • 135 patients eligible • Only 54 randomized • Non-randomized patients included for analysis • Primary endpoints • Mean BP and serum creatinine • 4 weeks and 6 months
Mean BP improved in medical and intervention arms during study period • Mean BP after angioplasty improved only in the bilateral, randomized group • Reduced hypertensive medication usage from 2.8 to 2.3 drugs in angioplasty groups • No differences in renal function between groups