RENAL ARTERY DOPPLER
RENAL ARTERY DOPPLER. Upon completion of the presentation the viewer should be able to: Identify a normal renal artery signal. Describe Tardus-Parvus, RAR and Acceleration index. List causes for hypertension Outline a normal Renal Doppler exam. Objectives.

RENAL ARTERY DOPPLER
E N D
Presentation Transcript
Upon completion of the presentation the viewer should be able to: Identify a normal renal artery signal. Describe Tardus-Parvus, RAR and Acceleration index. List causes for hypertension Outline a normal Renal Doppler exam Objectives
Indications for a Renal Doppler Exam Renal Artery Stenosis Hypertension Anatomy & Variants Diagnostic Criteria Doppler waveform Exam Protocol Case Examples Table of Contents
Evaluate a hypertensive patient for renal artery stenosis (RAS). Hypertensive patients not controlled with medical treatment. Patients with abdominal aortic dissection. Evaluation of renal transplant. Audible Bruit Patients with AAA Clinical Indications for Doppler
Renal Artery Stenosis:Causes • Atherosclerosis: Plaque deposits cause narrowing/blockage. • Affects men > women • Typically effects age >40 years • Involves proximal aspect renal artery • Fibromuscular: Fibrous tissue growth in arterial walls. • Affects women > men ( approx.. 4: 1). • Typically affects ages < 50 years • Involves mid to distal aspects of renal artery • Acute: Traumatic injury causing obstruction.
Relationship: Renal Artery Stenosis causes hypertension. Hypertension is the symptom that indicates RAS Doppler needed Hypertension and RAS
Hypertension and RAS Adrenal Gland Kidney
Hypertension and RAS • RAS • Increased PR • Decrease renal blood flow • Production of rennin
Hypertension and RAS • Rennin converts angiotensinogen to angiotensin. • Angiotensin is a potent vasonstrictor.
Hypertension and RAS • Angiotensin also acts on the adrenal cortex to produce aldosterone. • Aldosterone causes the kidney to absorbed more sodium and water.
Hypertension and RAS • This leads to increased in blood volume and also the BP.
Renal Artery Stenosis • Anatomy & Variants • Diagnostic Criteria • Doppler waveform • Exam Protocol • Case Examples
Kidneys Vessels Accessory Vessels Doppler Waveform Renal Anatomy
Size: 9-11cm Difference between Lt. & Rt. Renal Length < 2 cm Normal Anatomy of the Kidneys
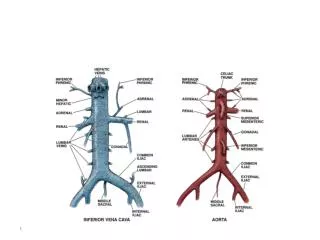
Celiac Axis Rt Renal Artery Lt Renal Artery Superior Mesenteric Artery Aorta
Segmental arteries Interlobar arteries Main Renal artery Arcuate arteries
Normal Right and Left Renal Artery Coronal View Transverse
Normal Right Renal Artery Transverse
Normal Left Renal Artery Transverse
Renal Artery Stenosis Normal Variants & Accessory Vessels
Normal Variants of Renal Arteries • Most common anatomy is single right and left renal artery (approx. 55% population)
Normal Variants of Renal Arteries • Second most common an is accessory renal artery branching off a main renal artery (14%)
Accessory Renal Arteries Branch off a main renal artery or aorta. Supply small portions of the renal parenchyma. Can be: 1) single or multiple 2) unilateral or bilateral
Accessory Renal Arteries • Can extend to upper, mid,or lower poles of kidney. • Stenosis in an accessory can result in hypertension. • Best evaluated in coronal plane with color Doppler.
Accessory Renal Arteries Two Left Renal Arteries
Low resistant waveform. Rapid and steep upstroke during systole. Dicrotic notch. Low resistant runoff during diastole. The Normal Renal Waveform
Diagnostic Criteria Protocol Example of normal Exam RAS Exam
Color Doppler non-visualization Peak Systolic Velocity RAR Acceleration time Acceleration Index End Diastolic Ratios Tardus Parvus Diagnostic Criteria
Peak Systolic Velocity • Normal >1.8 m/sec • Low grade(1-59%)>1.8 m/sec • No post-stenotic disturbance • High grade(60-99%)>1.8 m/sec • Post-stenotic turbulence • Total occlusion - no flow
Remember all angles MUST be 60 degrees or less! Peak Systolic Velocity
Renal-Aortic Ratio RAR = PSV renal artery PSV aorta
Renal-Aortic Ratio • PSV alone may be inaccurate due to difficulty with Doppler angle insonation • RAR angle independent • Obtain aortic signal 2cm distal to SMA • Use highest main renal artery signal
Renal-Aortic Ratio • Normal < 3.5 • Low grade (1-59%) < 3.5 • High grade (60-99%) > 3.5 • Total occlusion renal length < 9cm
End Diastolic Ratio • Assess both parenchymal vascular resistance and disease. • Sufficient perfusion: > 0.23 • Severe parenchymal vascular disease: < 0.23
Acceleration Index V AT T AI =V/ T
Acceleration Index • Acceleration time: time for peak systolic velocity • Acceleration index: acceleration slope divided change in time • < 3.78 kHz/sec/MHz indicates greater than 50% stenosis.
Acceleration Index • To calculate : • Place the first cursor at the beginning of systole. • Place the second cursor at the peak of systole.
Acceleration Time • Acceleration time: > 0.1 sec indicates greater than 50% stenosis. • Measure with sweep speed of 100 mm/sec. • Normal waveforms have steep systolic upstrokes, whereas waveforms distal to a stenosis have a more gradual upstroke and dampened systolic peak.
Abnormal Doppler Findings • Peak systolic velocity ( PSV) in renal artery ( proximal, mid, or distal ) > 180 cm/sec. • Renal Artery / Aorta Ratio ( RAR), > 3.5. • Tardus-Parvus.
What is Tardus-Parvus? • Tardus: delayed early systolic acceleration or upstroke • Parvus: diminished amplitude and rounding systolic peak.
What is Tardus-Parvus? Delayed upstroke
What is Tardus-Parvus? Rounded
Tardus-Parvus • Seen in distal & segmental arteries, indicating high grade stenosis proximally. • Measured using either : • Acceleration time (normal is less than 70ms) • Acceleration Index ( normal is greater than 3/m/s square) • When present, 100% indicative of RAS, but not ALWAYS present in RAS patients