Download

1 / 13
190 likes | 1.38k Vues
Renal Artery Stenosis. Major cause of renovascular hypertensionIncreasingly recognized as an important cause of chronic renal insufficiency and end-stage renal diseaseIn older individuals, atherosclerosis (AS) is by far the most common etiology of RASAs the renal artery lumen progressively nar

E N D
1. Renal Artery Stenosis Paul H. Tang, MD
2. Renal Artery Stenosis Major cause of renovascular hypertension
Increasingly recognized as an important cause of chronic renal insufficiency and end-stage renal disease
In older individuals, atherosclerosis (AS) is by far the most common etiology of RAS
As the renal artery lumen progressively narrows, renal blood flow decreases and eventually compromises renal function and structure
3. Pathophysiology Dyslipidemia, hypertension, cigarette smoking, diabetes mellitus, viral infection, immune injury, and increased homocysteine levels may contribute to endothelial injury
Endothelial changes leading to the formation of atherosclerotic plaques are very similar to those found in the other arteries
The resulting chronic ischemia produces adaptive changes in the kidney that are more pronounced in the tubular tissue
In patients with RAS, the GFR is dependent on angiotensin II and other modulators that maintain the autoregulation system between the afferent and efferent arteries and can fail to maintain the GFR when renal perfusion pressure drops below 70-85 mm Hg.
Significant functional impairment of autoregulation, leading to a decrease in the GFR, is not likely until arterial luminal narrowing exceeds 50%.
4. Mortality/Morbidity
The consequences are hypertension, and progressive loss of renal function (Ischemic Nephropathy).
In addition, the discovery of atherosclerotic RVD frequently occurs in the setting of generalized vascular disease (ie, cerebral, cardiac, peripheral), with the co-morbidity associated with disease in those vascular beds
Race: less common in African American patients
Sex: While the incidence of atherosclerotic RVD is independent of sex, Crowley et al showed that female sex (as well as older age, elevated serum creatinine level, coronary artery disease, peripheral vascular disease, hypertension, and cerebrovascular disease) is an independent predictor of RVD progression
5. Age: Studies have shown in hypertensive patients, 30% of patients have RAS, and the severity of stenosis increases with age
History:
progressive azotemia as a consequence of the renal ischemia and/or the persistence of significant hypertension
Refractory hypertension may occur
Physical:
The strong association of RVD with generalized AS indicates that any typical findings associated with cerebrovascular, cardiovascular, or peripheral vascular disease occur frequently in patients with RVD.
Abdominal bruits are highly specific for RVD when heard over the flank and are back-and-forth in nature
6. Patients with ischemic RVD present with one or more of the following clinical, historical, or diagnostic scenarios:
Azotemia occurs in patients with peripheral vascular occlusive disease, carotid or coronary artery disease, and other signs of AS.
Sudden worsening of hypertension or renal function may occur.
Acute renal failure or decreased renal function after antihypertensive therapy, especially with ACE inhibitors or angiotensin receptor blockers, may occur; an increase in serum creatinine levels of more than 15% in this setting is strongly suggestive of a high incidence of RVD.
Unexplained renal insufficiency may develop in elderly patients.
Congestive heart failure may occur with poor control of hypertension and renal insufficiency in the absence of a significant decrease in ejection fraction (the so-called flash pulmonary edema).
7. Causes: Risk factors associated with ischemic renal disease (IRD) are:
Hypertension: Of patients with IRD, 35% can be normotensive.
Advanced age: Most are found in 60-69 years old, and increases in persons older than 70 years.
Renal insufficiency
Extrarenal AS
Diabetes mellitus
Smoking
Lab Studies:
Serum creatinine levels to assess the level of renal dysfunction and can be used to calculate an estimated clearance based on Cockcroft-Gault equations or the MDRD formula developed by Levey et al.
8. Lab Studies (cont�d):
Perform a 24-hour urine collection to more accurately assess the level of renal dysfunction and to measure the degree of proteinuria. Vascular renal disease is more often associated with minimal-to-moderate degrees of proteinuria, which are rarely in the nephrotic range.
Urinalysis to ensure that red blood cells or red blood cell casts (a hallmark of glomerulonephritis) are absent.
Serologic tests for systemic lupus erythematosus or vasculitis if these conditions are suggested (eg, antinuclear antibodies, C3, C4, antinuclear cytoplasmic antibodies).
Peripheral renin activity reflects volume status in healthy individuals. It may be elevated in patients with renovascular causes of hypertension and in those with essential hypertension. It is equally nondiscriminatory in patients with atherosclerotic RVD with ischemic nephropathy.
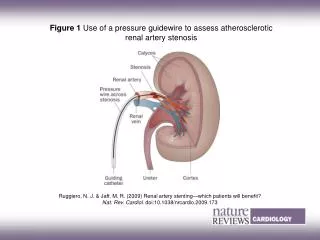
9. Imaging Studies:
Ultrasound
Renal ultrasound is performed frequently in patients with renal dysfunction.
Ultrasound is an anatomic, not a functional test.
Radionuclide scanning
Use of radionuclide scanning, is more useful in patients with normal renal function, in whom fibromuscular disease is suspected.
However results are unable to distinguish between parenchymal renal disease and RAS/ischemic nephropathy.
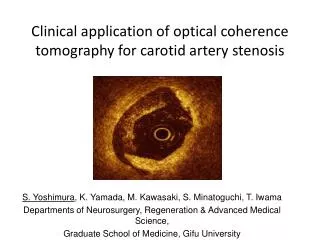
Duplex ultrasound scanning
Noninvasive diagnostic technique combining a B-mode ultrasound image with a pulse Doppler unit to obtain flow velocity data.
Relatively inexpensive, and can be used in patients with any level of renal function.
Sensitive and specific (98%)
With the use the renal resistance index value, the outcome of therapy in patients aggressively treated for RAS can be predicted
Spiral CT angiographt
Magnetic resonance angiography
Conventional arteriography
10. Imaging Studies (cont�d):
Contrast nephrotoxicity
Patients with progressive ischemic nephropathy should be informed of this risk prior to any contrast procedure.
Contrast nephropathy typically manifests as a brief rise in the serum creatinine level 3-6 days after exposure to radiocontrast.
Most patients with contrast nephropathy ultimately recover renal function.
Selection of diagnostic tests
Once patients are identified as being at high risk for RAS, the choice of the best test for diagnosis is controversial.
With standard noninvasive techniques accurate identification of patients with correctable renovascular hypertension can be difficult
invasive techniques with more accurate diagnostic potential can produce a worsening of renal function because of contrast toxicity and complications
11. The general approach to therapy of ischemic nephropathy involves control of hypertension, preferably with ACE inhibitors or angiotensin II antagonists. or, calcium channel blockers which are likely the most useful and best-tolerated agents. Initiate strict control of serum cholesterol, which usually requires the use of HMG-CoA reductase inhibitors, as with all conditions associated with AS.
All patients with significant (>80%) bilateral stenosis and stenosis in a solitary functioning kidney are candidates for revascularization, regardless of whether they have renal insufficiency. When renal insufficiency is present, patients with unilateral stenosis are also possible candidates for revascularization.
When renal function is normal or nearly normal (prevention of renal insufficiency), specialists recommend revascularization if the patient meets the following criteria:
The degree of stenosis is more than 80-85%.
The degree of stenosis is 50-80%, and captopril-enhanced scintigraphy findings demonstrate an activation of intrarenal RAS.
Medical Therapeutics
12. Medical Therapeutics Conversely, physicians can choose observation instead of revascularization when the patient meets the following criteria:
Stenosis is 50-80%, and scintigraphy findings are negative.
The degree of stenosis is less than 50%.
When renal insufficiency is present and the objective is recovery of renal function together with prevention of further renal function impairment, the prerequisites for revascularization are as follows:
The serum creatinine level is lower than 4 mg/dL.
The serum creatinine level is higher than 4 mg/dL but with a possible recent renal artery thrombosis.
When these conditions are satisfied, the authors propose revascularization if the following apply:
The degree of stenosis is more than 80%.
The serum creatinine level is increased after administration of ACE inhibitors.
The degree of stenosis is 50-80%, and the scintigraphy findings are positive.
13. Restrict conservative treatment in patients with an established diagnosis of IRD to those with absolute contraindications to surgery or angioplasty or to patients who are likely to succumb due to other comorbid conditions before advancing to end-stage renal disease.
Clinicians must rely on pharmacologic agents accepting the high probability of deterioration in renal function and shortened survival.
Surgical Care
Reports from retrospective studies clearly document that surgical revascularization can improve renal function in patients with ischemic nephropathy
Bypass procedures include aortorenal, hepatorenal, splenorenal, and iliorenal conduits constructed with autologous saphenous veins, autologous arteries, or prosthetic material.