BRAIN & SALT
BRAIN & SALT. Dr Mohammed Shamsah MBBS. FRCPC Chairman of Aneasthesia , Critical Care and Pain management Council State Of Kuwait 2011. Osmotherapy among Neurointensivest. 2011 (Angela et al) neurocrit care reported survey on Osmotherapy 295 responses 50% were neurologists

BRAIN & SALT
E N D
Presentation Transcript
BRAIN & SALT Dr Mohammed Shamsah MBBS. FRCPC Chairman of Aneasthesia, Critical Care and Pain management Council State Of Kuwait 2011
Osmotherapy among Neurointensivest • 2011 (Angela et al) neurocrit care reported survey on Osmotherapy • 295 responses • 50% were neurologists • Most used osmotherapy as needed either for ICH (89.9%) or cerebral oedema noted by imaging (54.9%) • Small minority reported using it prophylactically (16.8)
Osmotherapy • HTS 54.9% • Mannitol 45.1% • Reasons for preference include rebound oedema , duration of benefit , volume expansion rather than diuresis and lack of side effects • Those who preferred manniltol attributed to better experience and no need for central access • More neurosurgeons 61.9% used mannitol as to neurologists 44.9%
Osmotherapy • 28.1% used infusion of HTS others used either boluses or both • 65.9% prefare 3% saline • Some use Na acetate to Rx hyperchloraemic acidosis (more pronounced in fellows) • 67% reported target Na 150 – 160
Outline • Introduction • Physiology • Best evidence available • Complications • Conclusion
Outcome • For severe Injury (GCS<8) • 36% mortality • Quality of life (GCS<8) • Vegetative - 5% • Severe disability - 16% • Moderate disability - 16% • Good - 27%
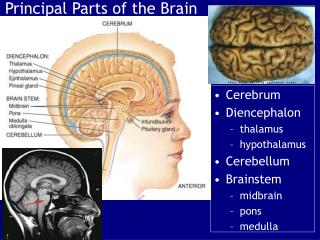
VOLUME REGULATION OF THE BARIN • ICP 8-12 mmHg • ICP > CVP and atmospheric pressure • To maintain ICP at normal level only small variations are accepted since the brain has a limited space for expansion • This control is largely achieved by the blood brain barrier (BBB)
Cerebral Blood Flow Regulation of Cerebral Vascular Resistance CBF Normal 50 - 100 ml / min PaCo2 (mmHg) MAP (mmHg) Normal 30 - 50 mmHg Normal 60 - 150 mmHg
BBB • Impermeable for solutes including small solutes Cl and Na and only water can pass
BBB Capillary Membrane • Protects the brain from transient changes in the blood biochemistry • Control interstitial milieu of the brain • Facilitates transfer of many substances by active transport • Permeability to water 30 times lower than in other organs but water passes freely • Na has a relatively high reflection coefficient
Forces are equal for fluid shift in all compartments (IF,ICF,Capillary) 5500mmHg = osmotic pressure created by small solutes similar to the size in plasma K Na ICF 5500 mmHg Cl PO4 2- ∆ Pc or Ponc --> filtered water In either direction according to The imbalance --> osmotic pressure in the opposite side --> Halting further fluid shift Only H2O IF 5500mmHg Pc = 20 - 30 mmHg Capillary P onc = 20 - 30 mmHg 5500 mmHg
Injured BBB Pc or P onc --> solutes and water filtered --> opposing osmotic pressure forces weaker . Always will be close to plasma/interstitium --> filtration is halted by increase in ICP K Na ICF Hypoxia causes intracellular oedema with no disturbance Of BBB --> no increase in Water content but redistribution 5500 mmHg Cl PO4 2- Small Solutes and H2O IF 5500mmHg Capillary 5500 mmHg Pc = 20 - 30 mmHg P onc = 20 - 30 mmHg
Haemodynamic effects of the rigid cranium Venous pressure outside dura 1 - 5 mmHg < tissue pressure inside dura (ICP) 10 - 12 mmHg Venous vessels collapse subdurally Degree of collapse depends on the pressure between ICP and Pout (RESISTOR) out upstream just before collapse = ICP RESISTOR protects the brain from variation in venous pressure out has to be greater than ICP to be transmitted to the brain Consequently head elevation should not affect ICP neither moderate increase in PEEP Head elevation reduces ICP by reducing CPP Venular resistance Arterial resistance
Haemodynamic effects of the rigid cranium • Filtration --> ICP --> venous collapse --> Pout upstream --> retrograde transmission of only 80 - 90% of the pressure Because of Rv --> increase filtration further • New steady state will be reached when ICP 8 - 9 times initial change in hydrostatic / oncotic pressure • This phenomena explains why small change in hydrostatic / oncotic pressure result in large change in ICP • Disturbed BB in Cats showed that change in arterial pressure will change ICP to the same extent as the initial change in • Arterial pressure (p < 0.05 and < 0.01) Venular resistance Arterial resistance
BRAIN: CEREBRAL EDEMA-CYTOTOXIC(Caused mainly by activation of cytokines, ROS and other pro-inflammatory mediators)
BRAIN: CEREBRAL EDEMA-VASOGENIC( Caused by Break down of BBB Caused mainly by activation of NMDA receptors by glutamate)
Oedema • Vasogenic :- caused by the break down of BBB • Cytotoxic :- cellular swelling of necrotic an apoptotic cells • Trauma has mixture of both • Initial mechanical injury and then secondary hypoxic injury
Effect of arterial and oncotic pressure variation on ICP • Auto regulation is important for the preservation of constant CBF • Disturbed BBB with loss of auto regulation will affect the hydrostatic pressure greatly thereby causing and increase in cerebral oedema that will only be stopped by increased ICP • Low oncotic pressure independent of auto regulation will increase filtration fraction that will only stop by an opposing increase in ICP
Cerebral Spinal Fluid • Produced by the choroid plexus • Average volume 90 - 150 ml • (0.35 ml / minute or 500 ml / day) • Reabsorbed through the arachnoid villi • Drainage may be blocked by inflammation of the arachnoid villi, diffuse cerebral edema, mass effect of hemorrhage or intraventricular hemorrhage
Patterns of Injury • Primary Injury • Occur at the moment of impact • Skin/Bones/Meninges/Brain/Blood vessels • Secondary Injury • Occur after impact • Expanding hematomas • Brain edema/swelling • Hypoxemia/Ischemia/Shock • Fever/infection • Electrolyte imbalance
MECHANISMS OF 2nd INJURY • Global • Hypoxia and ischemia of brain • Decreased cerebral blood flow due to increased intracranial pressure • Local • impairment of cerebral blood flow or extra cellular milieu due to the presence of injured brain
PATHOPHYSIOLOGY • Primary damage – the only treatment is by prevention. • Secondary damage – multifactorial and time dependent.
SOME of the SECONDARY EVENTS IN TRAUMATIC BRAIN INJURY diffuse axonal injury inflammation BBB disruption apoptosis necrosis edema formation Brain trauma ischemia energy failure cytokines Eicosanoids endocannabinoids Calcium polyamines Acetyl Choline ROS Shohami, 2000 Blue – pathophysiological processes; Yellow – various mediators
Dynamic Changes Following Stroke/Trauma Days Weeks / Months 2 7 8 hrs 14 Hours Ca,Na+Glut, ROS I N J U R Y Necrosis Apoptosis Inflammation RepairRemodeling Plasticity Functional Recovery Barone &Feuerstein JCBF, 1999
Surgery Decompression • Removing hematoma • Removing injured brain • Removing Bone/Foreign Bodies Fracture Repair Repair of Spinal Fluid Leak
Secondary Injury Expanding hematomas Brain edema/swelling Hypoxemia/Ischemia/Shock Fever/infection Electrolyte imbalance Seizures Coagulopathy Other non-neurologic (DVT, pneumonia…) Non-surgical Management
Let’s talk… • Guidelines of TBI • Mechanism of action of HS • Evidence available
Challenges & Limitations Summary statements Poor data Conservative Not always useful Can limit treatment Strengths Excellent concept Strong effort Big step towards standardizing care Blah blah… The Guidelines for the Management of Severe Closed Head Injury
HTS Mechanism Of Action • Osmotic • Haemodynamic • Vasoregulatory • Neurochemical • Immunologic
Osmotic • Increases osmotic gradient resulting in shift of fluid from interstitium to intravascular (more pronounced with intact BBB) • Counteract the effect of the accumulated extracellular osmolytes by increasing intravacular osmolarity to draw fluid from the interstitial space and thereby reducing ICP • Reduces CSF production
Haemodynamic • Increases CO • increases MAP • Smaller volumes therefore less overload and haemodilution
Vasoregulatory • Studies have shown that ischaemia causes secondary injury • Oedema , vasospasm and hyperperfusion (1st 2 weeksafter injury) are causes of ischaemia • HTS dehydrates endothelium and RBCs leading to increase diameter of vessels and movement of RBC. It also increases plasma volume counteract vasospasmand hypoperfusion by increasing CBF
Vasoregulatory • Stimulates autonomic nervous system to reduce central vascular resistance • Doyle et al 2001 : reported peripheral skin and muscle vasoconstriction secondary to vagal stimulation (mediated through lung osmo receptors) resulted in shunting of flow to the cerebral circulation • Reduces leukocytes adherence to endothelium • Releases endothelium relaxing factor and endothelin leading to vasodilatation • Releases prostocycline causing vasodilatation and inhibition of platelets aggregation (Seen human umbilical vein endothelial cells in vitro)
Vasoregulatory • Vagal stimulation causes release of atrial naturitic peptide causing moderate diuresis / naturesis . • Studies have shown that intraventricular administration of atrial naturitic peptide reduces ICP in rats with with global ischaemia/reperfusion model (Neurol res 1997)
Neurochemical • Increase Glutamate concentration extracellulary causes massive cell death • HTS prevents pathologic Glutamate release, since increased extracellular Na returns glutamate/Na pump to its normal glutamate reuptake function • Reduces intracellular Ca leading to less neuronal excitation • Restores Na, Cl , and resting membrane potential
Immunologic • Suppressive inflammatory effect • Reduces rate of infectious complications • Supresses CD4 suppression and normalizes natural killer cell activity in rat model • Limits amount of bacterial translocation
HTS for Resuscitation • Vasser Et al reported on 166 trauma patients undergoing helicopter transport in which SBP maintained > 110 mmHg with 7.5% HTS/4.2% dextran versus RL. • HTS group had less volume requirements for haemodynamic stabilization and higher SBP • Subgroup analysis showed better survival in the TBI subgroup Rx with HTS
HTS for Resuscitation • Vasser et al also reported in a different study that the addition of dextran to HTS did not improve outcome • In a meta-analysis (8 trials) performed by Wade et al comparing HTS/Dextran vs isotonic fluid resuscitation in hypotensive patients. There was an increased survival in the HTS/Dextran group P = 0.04 at 24hrs and to discharge
HTS for Resuscitation • Cooper et al in an RCT compared 7.5% HTS vs LR in the field (pre-hospital resuscitation bolus therapy of 250 ml plus additional fluids by paramedics) • 229 patients • No difference in total fluid requirements, SBP , ICP, CPP, inotropic support , and survival • This could be due to advanced pre hospital protocol that emphasized maintenance of adequate CPP
HTS and Intracranial Hypertension • Tseng et al in a case series of Poor Grade SAH • 23.5% HTS (2ml/kg/20 min) • ICP for 2 hrs • Cerebrovascularresisistance for 20 min • Increased CBF 20-50% in ischaemic area • Improved rheologyindices • Increased Na level by 11 meq/L and osmalality rose by 27 mOsm/L
HTS and Intracranial Hypertension • Vialet et al randomised 20 TBI patients to either 7.5% (2ml/kg) HTS or 20% mannitol • HTS Reduced number of episodes and duration of intracranial hypertension two times more effectively than mannitol , had a better osmotic load with a greater rise in osmalility . • No serious SE • 90 days outcome including mortality showed no difference • Confirms that increasing Na osmolar load could be more effective in treating high ICP