Download
1 / 41
460 likes | 732 Vues
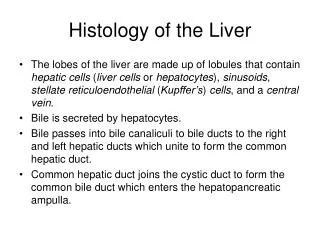
Machine preservation of the liver. Peter J Friend University of Oxford. Disclosure. I am co-founder and medical director of the Oxford University spin-out company, OrganOx, that has been set up to develop normothermic organ preservation. Centre G. Centre D. Centre E . Centre B. Centre F.

E N D
Machine preservation of the liver Peter J Friend University of Oxford
Disclosure I am co-founder and medical director of the Oxford University spin-out company, OrganOx, that has been set up to develop normothermic organ preservation.
Centre G Centre D Centre E Centre B Centre F Centre C Centre A Liver transplant survival – UK From transplantation
Centre G Centre D Centre G Centre E Centre B Centre F Centre C Centre B Centre A Centre F Centre D Centre E Centre A Centre C Liver transplant survival – UK From listing From transplantation Patients more likely to die on waiting list than postoperatively
Trends in liver transplantation • Increasing organ donation, but mostly in high risk donors • Increasing incidence of liver disease • Waiting lists increasing faster than transplants • Long waiting lists, restricted access, mortality The challenge – to transplant greater numbers of higher risk organs without compromising the outcome
Utilisation of donor livers 45% livers offered are accepted 76% livers accepted are transplanted (50% of DCD)
Limitations of static cold storage • Cooling • Loss of cell membrane functions • No oxygen delivery • Anaerobic metabolism • Accumulation of metabolites • Ischaemia-reperfusion • Limited viability assessment • Injury occurs at time of reperfusion Acceptable for high quality, but not marginal organs
DCD liver transplants have poorer outcomes Primary non-function Ischaemic cholangiopathy
Inferior outcomes - graft failure & biliary complications Patient Graft P<0.01 P<0.001 Foley. D’Alessandro et al et al 2011
Ischaemic cholangiopathy after DCD liver transplantation Success has been achieved at the price of selectivity
11 studies • Unrandomised control groups • 489 DCD (Maastricht 3) • 4455 DBD controls • Isch. cholangiopathy 16% vs. 3% (O/R 10.8) • Biliary complications 29% vs. 17% (O/R 2.4) • Retransplant (O/R 2.6) • Primary non-function (O/R 3.6) Jay, Skaro et al (2011), Northwestern, Chicago
Internalisation of membrane proteins during ATP depletion to reduce energy demand • Structural but lack of functional recovery after energy restoration (unlike renal tubular cells) Hepatology 2000, 31(5): 1045-54
Liver preservation – the key issues • Oxygen delivery • Machine perfusion (versus static) • Temperature
Am J Trans 2011, 11:2627-34 • Oxygen insufflation via IVC, exit via pin-pricks in capsule • Superior function; survival; transaminase release
(Rat liver reperfusion model) Trans Int 2010, 23: 944-50
Machine perfusion Hypothermic Normothermic
Pig DCD liver transplant model (60 min WI) 7 hr cold storage versus 6 hr CS + 1 hr HOPE Ann Surg 2009, 250 (5): 674-83
90 min warm ischaemia • 4 hours CS or HMP • Liver transplantation • Better immediate function with HMP • Progressive cellular injury • 20% survival Transplantation 2012, 94 (1): 22-29
Columbia University, New York Am J Trans 2010, 10: 372-381
Low risk donors • <65 yr, <25% steatosis, DBD • 20 HMP preserved organs (3-7 hr), matched controls • No difference in early histological appearances • Lower transaminase & lower cytokine expression in HMP Larger-scale clinical trial in progress
Normothermic machine perfusion Recreate physiological environment Physiological temperature Deliver oxygen Provide nutrients Allow normal metabolic activity Avoid ischaemia-reperfusion Assess viability
Survival after normothermic preservationDBD vs. DCD (40 min) DBD DCD
Normothermic DBD vs. DCD (40 min) ALT release DCD (n=6) DBD (n=7) P=NS
Viability assessment – Base excess DBD 5 hours DBD 20 hours DCD (40) 20 hours DCD (60) 20 hours * p<0.05 * * * *
Pig liver transplant model • 90 minutes warm ischaemia • 60 min normothermic recirculation (ECMO) • 4 hours normothermic preservation • 100% survival
Preservation or reconditioning? Recirculation Re-conditioning Organ retrieval Transplant Preservation Must the perfusion machine be transportable?
60 mins warm ischemia 4 hr UW 20 hours NP Liver retrieval Reperfuse 24 hr 24 hours NP
Bile output AST levels Base excess After 60 minutes warm ischaemia, 4 hours cold storage causes significant damage Reddy et al 2004
Pig liver DCD model • ATP levels • 30% after 60 min WI • 0% after 2 hr CS • 80% after 4 hr NMP J Surg Res 2011, 173: 83-88
From laboratory to clinic Commercial perfusion systems
Product specification: What matters? • Physical parameters: weight, size, materials • Usability: transportability, automation, ease of setup • Functionality (what features are essential?): • Blood or oxygen carrier? • In-line or off-line blood gas analysis? • Gas bottles or on-board gas production? • Mains power/DC power/battery power? • Parameters measured and displayed to the user? • Regulatory compliance • Cost
The OrganOx metra™ - start of perfusion Start After 10 secs After 60 secs Clinical trial in progress
Where will we be in 5 years? • Routine machine perfusion of all/most livers • Cold or warm? • Portable or static? • Logistic demands – retrieval teams • Cost implications • More donors and increased utilisation
Conclusions • Static cold preservation does not meet the challenges of marginal donor organs • Hypothermic machine perfusion • Benefits in pig model • Clinical studies in progress • Normothermic machine perfusion • Resuscitation, prolonged preservation & viability assessment (in pig models) • Cold preservation must be avoided (even in transit) • Clinical trials in progress Machine perfusion …. not whether, but how?