Download
1 / 48
480 likes | 760 Vues
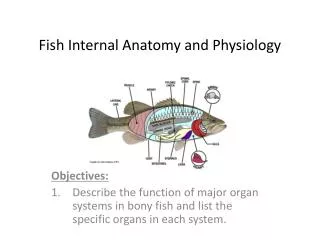
Chapter 24: Physiology of the Respiratory System. RESPIRATORY PHYSIOLOGY. Definition: complex, coordinated processes that help maintain homeostasis (Figure 24-1) 4 major functions: External respiration Pulmonary ventilation (breathing) Pulmonary gas exchange Transport of gases by the blood

E N D
RESPIRATORY PHYSIOLOGY Definition: complex, coordinated processes that help maintain homeostasis (Figure 24-1) 4 major functions: External respiration Pulmonary ventilation (breathing) Pulmonary gas exchange Transport of gases by the blood Internal respiration Systemic tissue gas exchange Cellular respiration Regulation of respiration
PULMONARY VENTILATION Respiratory cycle (ventilation, breathing) Inspiration: movement of air into the lungs Expiration: movement of air out of the lungs Mechanism of pulmonary ventilation The pulmonary ventilation mechanism must establish two gas pressure gradients (Figures 24-2 and 24-3) One in which the pressure within the alveoli (Pₐ) of the lungs is lower than atmospheric pressure (Pb) to produce inspiration One in which the pressure in the alveoli (Pₐ) of the lungs is higher than atmospheric pressure (Pb) to produce expiration
PULMONARY VENTILATION: MECHANISM Pressure gradients are established by changes in the size of the thoracic cavity that are produced by contraction and relaxation of muscles (Figures 24-4 and 24-5) Boyle’s law: the volume of gas varies inversely with pressure at a constant temperature Inspiration: contraction of the diaphragm and external intercostals produces inspiration; as they contract, the thoracic cavity becomes larger (Figures 24-6 and 24-7) Expansion of the thorax results in decreased intrapleural pressure, leading to decreased alveolar pressure Air moves into the lungs when alveolar pressure drops below atmospheric pressure Compliance: ability of pulmonary tissues to stretch, thus making inspiration possible
PULMONARY VENTILATION: MECHANISM (cont.) Expiration: a passive process that begins when the inspiratory muscles are relaxed, which decreases the size of the thorax (Figures 24-8 and 24-9) Decreasing thoracic volume increases the intrapleural pressure and thus increases alveolar pressure above the atmospheric pressure Air moves out of the lungs when alveolar pressure exceeds the atmospheric pressure The pressure between parietal and visceral pleura is always less than alveolar pressure and less than atmospheric pressure; the difference between intrapleural pressure and alveolar pressure is called transpulmonary pressure, always negative to avoid “collapse tendency of the lungs” Elastic recoil: tendency of pulmonary tissues to return to a smaller size after having been stretched; occurs passively during expiration
PULMONARY VENTILATION Pulmonary volumes: we must have normal volumes of air moving in and out as well as remaining in the lungs for normal exchange of oxygen and carbon dioxide to occur (Figure 24-11) Spirometer: instrument used to measure the volume of air (Figure 24-10) Tidal volume (TV): amount of air exhaled after normal inspiration, 500 ml Expiratory reserve volume (ERV): largest volume of additional air that can be forcibly exhaled past the TV(1000-1200 ml is normal ERV) Inspiratory reserve volume (IRV): amount of air that can be forcibly inhaled after normal inspiration (normal IRV is 3300ml) Residual volume: amount of air that cannot be forcibly exhaled (1200 ml)
PULMONARY VENTILATION (cont.) Pulmonary capacities: the sum of two or more pulmonary volumes Vital capacity (VC): the largest volume of air that can be moved in and out of the lungs; IRV + TV + ERV A person’s VC depends on many factors, including the size of the thoracic cavity and posture Functional residual capacity (FRC): the amount of air at the end of a normal respiration; ERV + RV Total lung capacity (TLC): the sum of all four lung volumes; the total amount of air a lung can hold Inspiratory capacity (IC): the maximal amount of air an individual can inspire after a normal expiration; TV + IRV Alveolar ventilation: volume of inspired air that reaches the alveoli Anatomical dead space: air in passageways that do not participate in gas exchange (Figure 24-6) Physiological dead space: anatomic dead space plus the volume of any nonfunctioning alveoli (as in pulmonary disease) Alveoli must be properly ventilated for adequate gas exchange
PULMONARY VENTILATION (cont.) Pulmonary air flow: rates of air flow into and out of the pulmonary airways Total minute volume: volume moved per minute (ml/min); TV x RR; 6000ml Forced expiratory volume (FEV) or forced vital capacity (FVC): volume of air expired per second during forced expiration (as a percentage of VC) (Figure 24-12) Flow-volume loop: graph that shows flow (vertically) and volume (horizontally), with the top of the loop representing expiratory flow volume and the bottom of the loop representing inspiratory flow volume relations (Figure 24-13)
Pulmonary Gas Exchange • Partial pressure – pressure exerted by one gas in a mixture • The partial pressure of a gas is related to the concentration of that gas in the mixture • In respiration we are concerned with the partial pressure of O2 and CO2 • Ex. The concentration of oxygen in the atm is 21% and the total pressure in the atm is 760mmHg, so Atm PO2 = 21% x 760 = 159.6mmHg • Gas will move from an area of high pressure to an area of low pressure
PULMONARY GAS EXCHANGE (cont.) Exchange of gases in the lungs: takes place between alveolar air and blood flowing through lung capillaries (Figures 24-15 to 24-17) Four factors determine the amount of oxygen that diffuses into blood The oxygen pressure gradient between alveolar air and blood The total functional surface area of the respiratory membrane The respiratory minute volume Alveolar ventilation Structural facts that facilitate oxygen diffusion from the alveolar air to the blood The walls of the alveoli and capillaries form only a very thin barrier for gases to cross The alveolar and capillary surfaces are large The blood is distributed through the capillaries in a thin layer so that each red blood cell comes close to alveolar air (Figure 24-18) Lung capillaries hold a large amount of blood
HOW BLOOD TRANSPORTS GASES Oxygen and carbon dioxide are transported as solutes and as parts of molecules of certain chemical compounds Hemoglobin (Hb) Protein found in RBC Composed of four polypeptide chains (two alpha chains, two beta chains), each with an iron-containing heme group CO2 can bind to amino acids in the chains, and oxygen can bind to iron in the heme groups (Figure 24-19) Transport of oxygen Oxygenated blood contains approximately 0.3 ml of dissolved O2 per 100 ml of blood vs. hemoglobin which contains about 20ml O2/100 ml Hb increases the oxygen-carrying capacity of blood (Figure 24-20)
HOW BLOOD TRANSPORTS GASES (cont.) Transport of carbon dioxide A small amount of CO2 dissolves in plasma and is transported as a solute (10%) Less than one fourth of blood CO2 combines with NH2 (amine) groups of Hb and other proteins to form carbaminohemoglobin (20%) (Figure 24-22) CO2’s association with Hb is accelerated by an increase in blood PCO2 (Figure 24-23) More than two thirds of the CO2 is carried in plasma as bicarbonate ions (70%) (Figures 24-24 to 24-26)
SYSTEMIC GAS EXCHANGE Exchange of gases in tissues takes place between arterial blood flowing through tissue capillaries and cells (Figure 24-27) Oxygen diffuses out of arterial blood because the oxygen pressure gradient favors its outward diffusion As dissolved oxygen diffuses out of arterial blood, blood PO2 decreases, which accelerates oxyhemoglobin dissociation to release more oxygen to plasma for diffusion to cells (Figure 24-28)
SYSTEMIC GAS EXCHANGE (cont.) • CO2 exchange between tissues and blood takes place in the opposite direction from oxygen exchange • Bohr effect: increased PCO2 decreases the affinity between oxygen and Hb (Figure 24-29) • Haldane effect: increased CO2 loading caused by a decrease in PO2
REGULATION OF PULMONARY FUNCTION Homeostasis of blood gases is maintained primarily by changes in inspiration Respiratory control centers: the main integrators controlling the nerves that affect the inspiratory and expiratory muscles are located in the brainstem (Figure 24-30) Medullary rhythmicity center: generates the basic rhythm of the respiratory cycle Consists of two interconnected control centers Ventral respiratory group – generates basic rhythm Dorsal respiratory group – integrates information from VRG and chemoreceptors
REGULATION OF PULMONARY FUNCTION (cont.) • The basic breathing rhythm can be altered by different inputs to the medullary rhythmicity center (Figure 24-30) • Input from the apneustic center in the pons stimulates the inspiratory center to increase the length and depth of inspiration • Pneumotaxic center in the pons inhibits the apneustic center and inspiratory center to prevent overinflation of the lungs
REGULATION OF PULMONARY FUNCTION (cont.) Factors that influence breathing: sensors from the nervous system provide feedback to the medullary rhythmicity center (Figure 24-31) Changes in the PO2, PCO2, and pH of arterial blood influence the medullary rhythmicity area PCO2 acts on central chemoreceptors in the medulla—if it increases, the result is faster breathing; if it decreases, the result is slower breathing A decrease in blood pH stimulates peripheral chemoreceptors in the carotid and aortic bodies and, even more so, stimulates the central chemoreceptors (because they are surrounded by unbuffered fluid) (Figure 24-32) Arterial blood PO2 presumably has little influence if it stays above a certain level
REGULATION OF PULMONARY FUNCTION (cont.) Arterial blood pressure controls breathing through the respiratory pressoreflex mechanism Hering-Breuer reflexes help control respirations by regulating depth of respirations and the volume of tidal air Cerebral cortex influences breathing by increasing or decreasing the rate and strength of respirations Ventilation and perfusion (Figure 24-33) Alveolar ventilation: air flow to the alveoli Alveolar perfusion: blood flow to the alveoli Efficiency of gas exchange depends on the ability to match appropriate alveolar ventilation and perfusion Efficiency of gas exchange can be maintained by limited ability to match perfusion to ventilation (e.g., vasoconstricting arterioles that supply poorly ventilated alveoli and allow full blood flow to well-ventilated alveoli)
THE BIG PICTURE: RESPIRATORY PHYSIOLOGY AND THE WHOLE BODY The internal system must continually acquire new oxygen and rid itself of CO2 because each cell requires oxygen and produces CO2 as a result of energy conversion Specific mechanisms involved in respiratory function Blood gases need blood and the cardiovascular system to be transported between gas exchange tissues of the lungs and various systemic tissues of the body Regulation by the nervous system adjusts ventilation to compensate for changes in oxygen or CO2 in the internal environment The skeletal muscles of the thorax help the airways maintain the flow of fresh air The skeleton houses the lungs, and the arrangement of bones facilitates the expansion and recoil of the thorax
Also… • Box • pp.811 Pneumothorax • pp.812 Types of Breathing • pp.818 CO poisoning • pp.825 Unusual Breathing Reflexes • pp.831 SIDS • Mechanisms of Disease • pp.830





![Respiratory Physiology [the Ins and Outs]](https://cdn2.slideserve.com/4330665/respiratory-physiology-the-ins-and-outs-dt.jpg)