Download
1 / 38
380 likes | 524 Vues
How can I help you? (or frequently asked questions). Adam Stacey-Clear Consultant Breast and Endocrine Surgeon. Who gets breast cancer?. Age Sex Where you live Family history Genetics Social class and alcohol. How common?. Incidence - 1 in 12 80% in women over 50 Very rare under 35.

E N D
How can I help you? (or frequently asked questions) Adam Stacey-Clear Consultant Breast and Endocrine Surgeon
Who gets breast cancer? • Age • Sex • Where you live • Family history • Genetics • Social class and alcohol
How common? • Incidence - 1 in 12 • 80% in women over 50 • Very rare under 35
Are there different types? • Ductal 85% • Lobular 15% • ER PR HER2 receptors • Basal, luminal phenotypes • Implications for rx
Screening • 50 years + • Every 3 years • Family history screening • Mammography • Ultrasound • MRI scans • Family history clinic/genetics
What treatments are available? • Surgery • Primary chemotherapy/endocrine therapy • Radiotherapy • Extended endocrine therapy (Tamoxifen, aromatase inhibitors) • Herceptin
Treatment side effects • Bone marrow supression • Aching joints • Switch to tamoxifen • Reassurance, SFO, low dose progesterones, venlafaxine ( flushes due to LHRH release) • Topical oestrogens • Menopausal status – blood tests (FSH)
How effective is treatment? Can it be cured? • CRC UK • 85% 5 year survival • 77% 10 year survival in England (2005-2009 data)
EBCTCG, Lancet 2011
Endogenous hormones • Early menarche, late menopause • Oophorectomy, antiestrogens • High plasma estrogens, high bone density • Postmenopausal obesity • Protective effect of pregnancy • Nulliparity, late first pregnancy Hormone-Related Events that Breast Cancer Risk
Mid 20th century – Standard endocrine therapy of oopherectomy for young patients and oestrogenic drugs for postmenopausal • 1962 – Tamoxifen (ICI 46,474) synthesised • Late 1960’s – first clinical studies of tamoxifen in advanced breast cancer patients at Christie Hospital, Manchester The history of endocrine therapy
1973 - ICI launch tamoxifen in ABC • 1992 - Oxford Overview confirm benefit of adjuvant TAM • 1995 - Anastrozole launched in ABC as 2nd line Rx • 2000 – AIs show benefit over TAM in 1st line ABC • 2002 – ATAC shows DFS benefit for adjuvant AIs over Tam • 2004 – Sequential AIs after TAM improve DFS & Survival The history of endocrine therapy
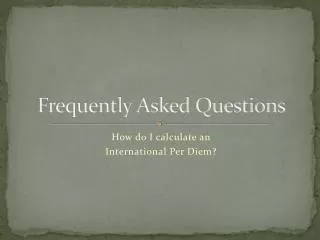
PRE-menopausal Women POST-menopausal Women Ovarlan Steroidogenesis AROMATASE ANDROSTENEDIONE Granulosa AROMATASE Adipose Tissue Liver Breast Breast Tumor Corpus Luteum Adrenal Gland Estrogen Stimulation of Target Tissues Target Tissues eg, BREASTBREAST TUMOR ESTRADIOL ESTRADIOL ESTRONE
Aromatase Inhibitors Anastrazole, Exemestane, Letrozole POST-menopausal Women Tamoxifen Faslodex ANDROSTENEDIONE AROMATASE Adipose Tissue Liver Breast Breast Tumor Adrenal Gland Estrogen Stimulation of Target Tissues Target Tissues eg, BREASTBREAST TUMOR ESTRADIOL ESTRONE
All post menopausal pts with node positive disease should be offered Letrozole after completing 5 years of tamoxifen. • With no clear benefit appearing for different strategies then side effects and costs are important considerations. • We recommend switching to an aromatase inhibitor after 2-3 years of tamoxifen or vice versa for all postmenopausal node negative pts. • Skeletal health should be monitored as per recommendations. • Up front AIs should be considered for post menopausal pts who are Her-2-neu positive? node+ve and those with contraindications to tamoxifen. Recommendations
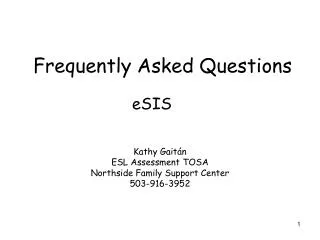
Efficacy Endpoints Favors Exemestane Favors Tamoxifen HR (95% CI) Disease Free Survival 0.76 (0.66, 0.88) ITT (E=354, T=454) ER+/UNK (E=339, T=438) 0.75 (0.65, 0.87) Breast Cancer Free Survival ITT (E=289, T=374) 0.76 (0.65, 0.88) ER+/UNK (E=277, T=361) 0.75 (0.64, 0.87) Time to Distant Recurrence 0.83 (0.70, 0.98) ITT (E=249, T=297) ER+/UNK (E=238, T=285) 0.82 (0.69, 0.98) Time to Contralateral BC 0.57 (0.33, 0.98) ITT (E=20, T=35) 0.56 (0.33, 0.98) ER+/UNK (E=20, T=35) 0.4 0.6 0.8 1.0 1.2 Coombes RC, et al. Data presented at ASCO, June 2006 Hazard ratio (95% CI)
CRC UK trial tamoxifen alone v surgery and tamoxifen • 451 women 70 years or over • 34 months FU • no significant early differences in survival or quality of life follow-up • significantly higher loco-regional relapse rate with tamoxifen alone [23% v 8%] Tamoxifen Alone v Surgery + Tamoxifen:‘Golden Oldies’ Bates et al Br J Surg 78:591-594, 1991
Routine calcium and vitamin D supplements • “Baseline” DXA in all patients beginning 5 years of an AI • If osteoporosis - give approved bisphosphonate • If osteopaenia - monitor annually • Treat if confirmed bone loss of >5% per year • If normal - monitor every 2-3 years • “Baseline” DXA in over 65s receiving TAM - AI sequential therapy • Monitor and treat as above • “Baseline” DXA in all patients with premature (<45) menopause • Monitor and treat as above Provisional Recommendations “Baseline” = within 3 months of initiating AI/ inducing menopause
Baseline DEXA scan and risk assessment if for AI therapy • Risk adapted strategy • Lifestyle advice and adequate calcium and vitamin D • 1 g calcium and 800iu vitamin D • Reassure if T score > -1 and no risk factors • No monitoring required • Monitor BMD of osteopaenic patients every 2 years • Baseline T score <-1 • Intervention with bisphosphonates • > age 75 and > 1 risk factor for osteoporotic fracture • T score < -2 either at baseline or on follow-up • T score < -1 at baseline and annual bone loss >4% UK Management Algorithm for Breast Cancer - NOS/NCRIPost-menopausal women >age 45
5 years tamoxifen= £136 • 5 years AI =£5400 • 2yrs Tamoxifen 3yrs AI=£3294 • 3yrs Tamoxifen 2yrs AI=£2241 Issues-Costs
Encodes a 185kd protein that is a member of the type I receptor tyrosine kinase family which also contains EGFR, HER-3 and HER-4 Functions When Altered • Growth and proliferation increased • Differentiation decreased • Cell survival increased • Motility increased • Neoangiogenesis increased • Reduced dependency on estrogen and insensitivity to hormonal blockade The HER-2 Gene
Combined Analysis for DFS of NSABP B-31 / NCCTG – N9831 ACTH 87% 85% ACT 75% % 67% N Events ACT 1679 261 ACTH 1672 134 HR=0.48, 2P=3x10-12 Years From Randomization
Combined Analysis for DDFS of NSABP B-31 / NCCTG – N9831 100 ACTH AC->T+H 90% 90% 90% 90% 90% 90% 90 ACT AC->T 80 81% 81% 81% % 74% 74% 74% 70 N Events N Events ACTH 1672 96 ACT 1679 194 AC->T 1679 194 60 AC->T+H 1672 96 HR=0.47, 2P=8x10-10 HR=0.47, 2P=8x10-10 50 0 1 2 3 4 5 Years From Randomization
Annual Hazard of Distant Recurrence 120 100 ACT 80 Rate per 1000 Women /Yr 60 40 ACTH 20 0 0 1 2 3 4 Years From Randomization
Summary • Dramatic improvements in DFS • Early overall survival benefit • Optimal duration Unknown (HERA 1 vs. 2y pending). Current data supports one year (9weeks?) • ? Concurrent better efficacy but assoc with xs cardiac events • Assessment of cardiac ftn. remains important
‘Evolution’ of Chemotherapy ) 100 Dose Dense FEC - D 83% 83% TAC 78% 78% AC - T 75% 75% Adriamycin 67% 67% CMF Surgery % relapse free 50 3 5,9 % 3 5,9 % 3 2,4 % 3 2,4 % 2 6% 2 6% 0 1 3 5 7 9 11 1 3 15 1 3 5 7 9 11 1 3 15 Time (years)
Early Results Do Not Always Reflect Late Results In Adjuvant Therapy Poly Chemotherapy Tamoxifen (5 yrs) Proportional Risk Reduction During Time Interval Time Periods (yrs) Time Periods (yrs) Recurrence Breast Cancer Specific Mortality
Breast conserving surgery + RT v. BCS alone - Ipsilateral breast recurrences
Breast conservation + RT v. mastectomy - breast cancer deaths
Adjuvant radiotherapy following mastectomy – benefit additive to chemotherapy Overgaard et al. NEJM 1997
Follow up • Bone density scans every 2 years if on aromatase inhibitor • Mammography • Ultrasound • Local recurrence – 72% between clinic visits
Thyroid cancer • V rare – less than 1% of all malignancies • Women more than men • Solid lump in male more worrying • Nuclear medicine scan • Ultrasound guided FNA • Blood tests
Thyroid types • Follicular • Papillary • Medullary • Anaplastic • Total thyroidectomy or partial thyroidectomy? • Nuclear medicine imaging • Auto antibodies • Thy 1 – Thy 5 • CT scans
Thyroid cancer prognosis • Very good even with lymph node metastasis • 97% 10 year survival • Thyroglobulin measurements • Long term follow up
Thyroid surgery • Recurrent laryngeal nerve injury • Hypocalcaemia • Hypothyroidism • Length of stay • Follow up – annual blood tests • Pregnancy
Thyrotoxicosis • 60% relapse on medical treatment eg carbimazole or propylthiouracyl • Antibodies • Radioiodine ablation – age, exophthalmos, local preferences • Surgery – usually curative • Lifelong thyroxine