Download
1 / 54
540 likes | 699 Vues
Role of anesthetist in neurointensive management of head trauma. Dr Megha Jain. University College of Medical Sciences & GTB Hospital, Delhi. Head Injury. Leading cause of permanent disability & death Most frequent in adolescents & young adults ( 15 – 30 yrs. )

E N D
Role of anesthetist in neurointensive management of head trauma Dr Megha Jain University College of Medical Sciences & GTB Hospital, Delhi
Head Injury • Leading cause of permanent disability & death • Most frequent in adolescents & young adults ( 15 – 30 yrs. ) • Incidence per year in US is around 200/1 lakh population • Corresponds to 5 lakh individuals ( 50,000 die prior to hospitalization ) • Males affected twice more commonly • Usually associated with multiple injuries resulting in significant blood loss, hypotension & hypoxia • Prognosis depend on type of lesion, age of patient, severity of injury & associated features like hypoxia, hypercarbia & hypotension
Classification of head injury Primary injury Produced by direct mechanical impact Result in skull fractures & intracranial lesions Diffuse brain injury Focal brain injury Concussion Contusion Epidural hematoma Subdural hematoma Axonal injury Intracerebral hematoma
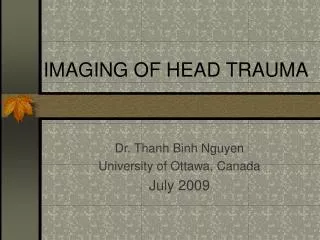
Epidural Hematoma Due to tear in middle meningeal vessels or dural sinuses LOC + Lucid interval may be + Subdural hematoma Caused by tearing in bridging veins b/w cerebral cortex & draining sinuses C/F Ranges from minimal deficits to LOC Signs of mass lesion ( hemiparesis, pupillary enlargement ) Lucid interval may be + Symptoms within 72 hrs – Acute, in b/w 3 - 15 days - Subacute, after 15 days – Chronic.
SUBDURAL HEMATOMA EPIDURAL HEMATOMA
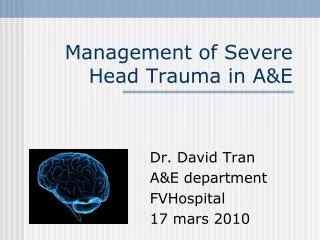
Intracerebral hematoma: Common in coup & counter coup injuries Usually located in frontal & temporal lobes Visualized as hyperdense mass on CT scan C/F Minimal neurological deficit to deep coma Intensive medical therapy to manage cerebral edema & Control ICP . Diagnosis – CT scan & MRI, Emergency evacuation in all three TEEMPORAL INTRACEREBRAL HEMATOMA
Classification of head injurycontd…. • Secondary brain injury Develops within minutes to hours of initial injury Cause further damage to nervous tissue Caused by the following: • Respiratory dysfunction – hypoxemia, hypercarbia • Cardiovascular instability – hypotension, low cardiac output • Elevation of ICP • Biochemical derangements
Classification of head injury contd…. Based on GCS in terms of severity MILD 13 – 15 MODERATE 9 – 12 SEVERE </= 8
Systemic sequelae of head injury • Cardiovascular response to head trauma In early stages – hypertension, tachycardia & ↑ CO ( due to symp. Stimulation ) But eventually due to multiple injuries & substantial blood loss Hypotension ↓ CO Shock
Systemic sequelae contd…. • Respiratory problems - Airway obstruction - Hypoxemia - ARDS ( trauma related ) - Neurogenic pulmonary edema - Apnea & abnormal respiratory patterns - Aspiration, pneumonia
Systemic sequelae contd…. Neurogenic pulmonary edema • Rapid onset, marked pulmonary congestion & intraalveolar hemorrhage & accumulation of protein rich edema fluid. • Result from massive sympathetic discharge from injured brain secondary to intracranial hypertension. • Therapy consists of Immediate medical or surgical relief of ↑ ICP Supportive respiratory care Careful fluid management
Systemic sequelae contd…. • Temperature regulation: May be disturbed & hyperthermia, if it occurs, can provoke further brain damage • Clotting abnormalities: DIC may occur due to release of brain tissue thromboplastin into systemic circulation • Gastrointestinal problems- Stress ulcer, hemorrhage may occur after 3 – 4 days.
Systemic sequelae contd…. • Endocrinologic problems: Post. Pituitary dysfunction – frequent DIABETES INSIPIDUS may occur after craniofacial trauma & basal skull fracture C/F polyuria, hypernatremia, high serum osmolarity, dilute urine. Frequently it is transient T/T – water replacement - Exogenous vasopressin administration
Systemic sequelae contd…. • Endocrinologic problems: SIADH: Hypernatremia, Urine osmolarity > Serum osmolarity C/F Anorexia, nausea, vomiting, Irritability, personality changes ( due to water intoxication ) Usually seen 3 – 15 days after trauma T/T – water restriction
Systemic sequelae contd…. • Changes in cerebral circulation & metabolism: Acute brain swelling – provoked by ↓ in vasomotor tone Cerebral edema – mixture of vasogenic & cytotoxic types caused by blood brain barrier disruption & ischemia. Intracranial hypertension Herniation of brain stem through foramen magnum
Systemic sequelae contd…. • Changes in cerebral autoregulation: Frequently impaired, ↑ ing the risk of brain injury with sudden changes in systemic blood pressure Elevation in BP - ↑ risk of vasogenic edema, ↓ in BP - may result in cerebral ischemia.
Changes in cerebral autoregulation In the presence of head injury or subarachnoid hemorrhage, inadequate cerebral perfusion can occur even with reasonable, normotensive blood pressures. Even slight hypotensive responses are sufficient to promote cerebral ischemia.
Autoregulation testing methods • Spontaneous relationship b/w blood pressure & flow velocity changes - intact cerebral autoregulation – there is negative correlation b/w blood pressure & change in flow velocity, - impaired cerebral autoregulation – the correlation is positive • Transient hyperemic response – - compression of extra cranial internal carotid artery for 7 – 10 seconds results in transient hyperemic response in the ipsilateral middle cerebral artery if cerebral autoregulation is intact.
Autoregulation testing methods • Dynamic autoregulation: - intact autoregulation – transient ↓ in BP causes a very brief ↓ in middle cerebral artery flow velocity, rapidly returning to baseline value • Static autoregulation: - intact autoregulation – elevation of systemic BP using a vasopressor ( phenylephrine ) will not affect cerebral artery flow velocity.
Initial assessment and resuscitation • Rapid overview- in few seconds - to determine whether pt. is stable or unstable. • Primary survey – evaluation & concurrent resuscitation - Airway – patency, F.B - Breathing – spontaneous, adequacy - Circulation – HR, BP, Peripheral pulses - Neurological function – quick assessment.
AVPU System • A = Alert. • V = Responds to verbal stimuli. • P = Responds to painful stimuli. • U = Unresponsive.
Glasgow Coma Scale • EYE OPENING: Spontaneously 4 To verbal command 3 To pain 2 None 1 • BEST VERBAL RESPONSE: Oriented, conversing 5 Disoriented, conversing 4 Inappropriate words 3 Incomprehensible sounds 2 No verbal response 1
Glasgow Coma Scale • BEST MOTOR RESPONSE: Obeys verbal commands 6 Localizes pain 5 Flexion/withdrawal 4 Abnormal flexion ( decorticate ) 3 Extension ( decerebrate ) 2 No response ( flaccid ) 1
Assessment contd…. • Pupillary response – - Dilated & sluggishly reacting pupil – suggests compression of 3 rd nerve by medial portion of temporal lobe ( uncus ) After preliminary assessment & management of the patient secondary survey should be done • Secondary survey Systemic examination, rule out intrathoracic & intrapelvic hemorrhage Rule out associated injuries
Intubation issues: Risks and benefits Intubation in principle protects against aspiration/regurgitation of stomach contents if airway reflexes are compromised secondary to injury. Also,CO2 retention as a result of diminished ventilatory drive and/or soft-tissue obstruction of the upper airway may occur. Increased CO2 retention can lead to increase cerebral blood flow & blood volume, factors which result in ICP elevation. However intubation can result in raised ICP
Establishment of Airway & Ventilation contd.. • All trauma patients are considered to have a full stomach & frequently ( approx 10 % ) have an associated cervical spine injury as well Cricoid pressure & MILS are used during laryngoscopy & intubation
Establishment of Airway & Ventilation contd.. • The following sequence would apply: • preoxygenation • cricoid pressure for esophageal occlusion • brief general anesthesia induced using IV thiopental (3-4 mg/kg) and lidocaine (1.5 mg/kg) and muscle relaxation by succinylcholine (1.5 mg/kg). • Following attainment of the secure airway, hyperventilation to a PaCO2 of about 30 mm Hg should be initiated
Establishment of Airway & Ventilation contd.. Contraindications to the application of cricoid pressure are: • Suspected airway injury (especially injuries at the cricotracheal junction). • Foreign body at the level of the cricoid (either within the esophagus or the trachea). • Active vomiting. • Awake intubation or lightly sedated patient.
Establishment of Airway & Ventilation contd.. Contraindications to nasal intubation Suspected skull base fracture Severe facial injuries Bleeding diathesis
Alternative techniques to secure airway Laryngeal Mask Airway (LMA) As well as maintaining the airway, a tracheal tube (size 6 or less) may be placed, either blindly or via flexible fibreoptic laryngoscopy. The LMA does not however protect the airway from aspiration Proseal LMA
Alternative techniques contd.. Intubating LMA Advantage: even 8 mm ET tube can be passed Disadvantage: its metal part can exert pressure against cervical vertebrae. Combitube The Combitube is a double lumen tube inserted blindly into the oesophagus or trachea. The position of the tube is confirmed by the presence of breath sounds or capnography. By inflating one of the two cuffs present, the lungs may then be ventilated.
Alternative techniques contd.. CricothyroidotomyThe need for a surgical airway should be recognised quickly and performed by an experienced person without delay. It may be used as a primary airway, with injuries to the maxillofacial area or after failure of orotracheal intubation. The potential for carbon dioxide retention with this technique must be remembered and the levels in arterial samples monitored.
Alternative techniques contd.. Tracheostomy Takes longer time Require neck extension, can exacerbate cord trauma in patients with cervical spine injuries Considered after 2 – 3 days of cricothyroidotomy
Cardiovascular stabilization • Systemic hypotension – major contributor to poor outcome Fluid resuscitation: Hypovolemia often masked by stable BP secondary to sympathetic overactivity or reflex response to raised ICP. Thus Urine output & CVP should be used as guide. Crystalloid & colloid solutions Isotonic & hypertonic solutions are preferred Hypertonic saline ( 3 % ) may be beneficial Hestarch maintains intravascular volume for longer period but interferes with coagulation
Cardiovascular stabilization • Blood & blood products Maintain hematocrit above 30 % Improves oxygen delivery • Avoid glucose containing solutions • Inotropes & vasopressors ( dopamine ) to maintain CPP above 60 mmhg
Monitoring in patients with head injury Standard monitoring : HR, Rhythm, ECG, NIBP/IBP, sPo2, ETCO2, Temp. Urine output, CVP, NMB, ABG, Hematocrit, Glucose, Electrolytes, Serum osmolarity, Urine osmolarity. Brain monitoring : EEG, Evoked potential, Jugular venous oxygen saturation, Brain tissue PO2, ICP.
Influence of intracranial hematoma on ICP and CPP Mass effects of expanding intracranial hematomas results in local and general increases in brain pressure, which causes hemodynamic alterations such as (a) reduced cerebral perfusion pressure and (b) reduced brain blood flow.
Clinical manifestations of increased ICP • Headache, nausea & vomiting, somnolence, papilledema, and blurred vision. • CT scan findings consistent with ICP elevation include Midline shift, Loss of sulci, Ventricular effacement (if hydrocephalus is present, ventricular enlargement may be observed), Edema. On CT scans, edema appear black (hypodense)
ICP monitoring: Indications- (1) Patients with significant head injury (Glasgow Coma Scale 3-8 following resuscitation) (2) Abnormal CT scan revealing contusion, edema, hematoma, compressed basal cisterns. (3) Patient exhibits severe head injury but has a normal CT scan; however, two or more of the following findings are present at admission: Age > 40,abnormal posturing, systolic hypotension ( </= 90 mmhg )
Approaches for intracranial pressure monitoring • Catheter tip strain gauge or fiber-optic units are most often used, calibrated before insertion. • Placement: lateral ventricles, parenchyma [using catheter tip pressure transducers], subdural, subarachnoid, or epidural spaces.
Management of elevated ICP • Posture – HEAD UP TILT 10 – 30 degree helps in CSF drainage • Hyperventilation to a PaCO2 of 30 mmhg in cases where transtentorial herniation exist • Diuretic therapy – Mannitol 1 g/kg i/v over 10 - 20 minutes - Furosemide 0.1 to 0.2 mg/kg • CSF drainage by a catheter. • Barbiturates – cerebroprotective , but hemodynamic stabilization is a prerequisite • Steroids have no proven role
Head Position vs ICP & CPP As head-up position is increased, ICP may be reduced, but beyond 30* heads-up CPP is likely compromised.
Jugular venous oxygen saturation Provides information about balance b/w global cerebral oxygen delivery & metabolic demand Retrograde placement of jugular venous catheter equipped with an oximeter into the jugular bulb can provide continous measurement of SJVO2 On lateral skull x ray catheter tip should be at the level of & just medial to the mastoid process
Jugular venous oxygen saturation Normal SJVO2 – 55 to 75 % SJVO2 < 55 % suggest cerebral hypoperfusion SJVO2 > 80 % suggest cerebral hyperemia caused by raised CBF
Brain tissue oxygen pressure Measured continously with a small flexible microcatheter inserted into brain parenchyma Provide regional measurement & can be inserted into brain tissues considered to be at risk Normal values are 25 – 30 mmhg Values < 15 mmhg – poor prognosis Values < 10 mmhg – incompatible with life.
Nutrition Feeding usually begins within 72 hrs. of injury in order to achieve full nutritional support Feeding protocol : 50 kcal/kg/day Protein content : 15 % of total calories Enteral route is better Parenteral route : expensive, increased risk of infection & gut atrophy Immune enhancing, immune modulating diets containing glutamine, arginine, omega 3 fatty acids are beneficial
Antiseizure prophylaxis Incidence of seizures following TBI is about 50 % Anti convulsants are indicated to prevent early ( within 7 days ) post traumatic seizures but not for late ones
DVT Prophylaxis Use of graduated compression stockings or intermittent pneumatic compression stockings have been recommended in patients with severe TBI Use of prophylactic LMWH has also been recommended However its use increases the risk of intracranial bleed
General nursing care Positioning When positioning the unconscious patient, proper body alignment should be maintained. Limbs must be supported in a position of function. When turning the patient, alignment should be maintained and log rolling should be done The patient's position should be changed to a new weight-bearing surface every two hours. This decreases the likelihood of complications such as decubitus ulcers, orthostatic pneumonia, and thrombophlebitis.