Acute Bacterial Meningitis
540 likes | 731 Vues
Acute Bacterial Meningitis . DEMOGRAPHY AND EPIDEMIOLOGY. The highest incidence is among neonates, who are usually infected by bacteria found in the birth canal at the time of parturition.

Acute Bacterial Meningitis
E N D
Presentation Transcript
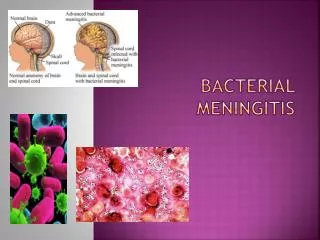
DEMOGRAPHY AND EPIDEMIOLOGY • The highest incidence is among neonates, who are usually infected by bacteria found in the birth canal at the time of parturition. • Group B streptococci (Streptococcus agalactiae) account for the majority of cases; other causes include Listeria monocytogenes, E.coli, other Gram-negative bacilli, and enterococci. • From age 1 to 23 months, the most common organisms are Streptococcus pneumoniae and Neisseria meningitidis
Children from the second to the fifth year used to have a high rate of infection caused by Haemophilus influenzae type b. However the wide use of protein-polysaccharide conjugated vaccines has dramatically reduced the incidence of this infection • From age 2 through 18, N. meningitidis is the most common cause, accounting for more than one-half of cases, followed by S. pneumoniae • In adults up to age 60, S. pneumoniae is most common followed by N. meningitis • Over age 60, most cases are due to S. pneumoniae and less often L. monocytogenes
Etiology - in Adults • S. pneumoniae 30-50% • N. meningitidis 10-35% • H. influenzae 1-3% • G -ve bacilli 1-10% • Listeria species 5% • Streptococci 5% • Staphylococci 5-15%
Predisposing factors • Most cases of meningitis occur when colonization by potential pathogens is followed by mucosal invasion of the nasopharynx • However, some patients develop disease by direct extension of bacteria across a skull fracture in the area of the cribriform plate • Other patients develop meningitis following systemic bacteremia as with endocarditis or a urinary tract infection or pneumonia • Other predisposing conditions include asplenia, complement deficiency, corticosteroid excess, and HIV infection
Etiology and epidemiology of meningitis • Lack of immunity ( IgM or igG anti capsularantibody ) to specific pathogens with young age. • recent colonization with pathogenic bacteria . • Close contact with invasive disease ( respiratory tract secration) • Crowding , poverty , black race , male . • Defect in complement (C5- C8 ) associated with recurrent meningococcal infection .
Etiology and epidemiology of meningitis • ventricular-peritoneal shunts: Coagulase negative staphylococci and corynebacteria . • CSF leaks due to fracture cribriform palate or paranasal sinus ( pneumococcal ).
Etiology and epidemiology of meningitis • Splenic disfunction (sickle cell anemia or asplenia ) increased risk of pneumococcal , H.influenza type b ,rarely meningococcal sepsis and meningitis . • . • head trauma or neurosurgical procedures ( staphylococci )
Etiology and epidemiology of meningitis(con) • Immuno-suppressed patients with T-cell defects (AIDS, and malygnancy) : Cryptococcal and L.monocytogens. • Open neural tube defect : Meningomyelocele and lombosacral dermal sinus associated with staphylococci -Aureus and gram – negative
CLINICAL FEATURES • The overwhelming majority of patients with bacterial meningitis have fever and headache • Most patients have high fevers, but a small percentage have hypothermia • CNS symptoms • Some patients will have significant photophobia and/or clouding of the sensorium • Changes in mentation and level of consciousness, seizures, and focal neurologic signs tend to appear later in the course of disease
CLINICAL FEATURES • Nuchal rigidity • Passive or active flexion of the neck will usually result in an inability to touch the chin to the chest • Tests to illustrate nuchal rigidity • The Brudzinski sign refers to spontaneous flexion of the hips during attempted passive flexion of the neck • The Kernig sign refers to the inability or reluctance to allow full extension of the knee when the hip is flexed 90 degrees
CLINICAL FEATURES • Other findings • Some infectious agents, particularly N. meningitidis, can also cause characteristic skin manifestations, petechiae and palpable purpura • If meningitis is the sequela of an infection elsewhere in the body, there may be features of that infection still present at the time of diagnosis of meningitis eg, otitis or sinusitis
Differential Dx • Viral- 40 % of meningitis • Fungal • Tuberculous • Spirochete • Chemical / Drug induced • Collagen Vascular Disease • Parameningeal infection: brain abscess, epidural abscess • Subarachnoid hemorrhage • Neuroleptic Malignant Syndrome
LABORATORY FEATURES • Most often the WBC count is elevated with a shift toward immature forms • Platelets may be reduced if disseminated intravascular coagulation is present or in the face of meningococcal bacteremia • Blood cultures are often positive, and can be very useful in the event that CSF cannot be obtained before the administration of antimicrobials • At least one-half of patients with bacterial meningitis have positive blood cultures, with the lowest yield being obtained with meningococcus
LABORATORY FEATURES • CSF analysis – every patient with meningitis should have CSF obtained unless the procedure is contraindicated • Chemistry and cytologic findings highly suggestive of bacterial meningitis include a CSF glucose concentration below 45 mg/dL, a protein concentration above 500 mg/dL, and a white blood cell count above 1000/mm3 • A Gram stain should also be obtained • The Gram stain is positive in up to 10 percent of patients with negative CSF cultures and in up to 80 percent of those with positive cultures
Opening pressure>180 mmH2O White blood cells10/ L to 10,000/ L; neutrophils predominateRed blood cellsAbsent in nontraumatic tapGlucose <2.2 mmol/L (<40 mg/dL)CSF/serum glucose <0.4Protein>0.45 g/L (>45 mg/dL) Gram's stainPositive in >60%CulturePositive in >80% Latex agglutinationMay be positive in patients with meningitis due to S. pneumoniae, N. meningitidis, H. influenzae type b, E. coli, group B streptococci Limulus lysatePositive in cases of gram-negative meningitisPCRDetects bacterial DNA
Typical Cerebrospinal Fluid Findings in Patients with Bacterial Meningitis
Complications of Meningitis One of the most common problems resulting from meningitis is hearing loss.Anyone who has had meningitis should take a hearing test. • Young children: • Babyish behavior • Forgetting recently learned skills • Reverting to bed-wetting • Babyish behavior
Older people: • Lethargy • Recurring headaches • Difficulty in concentration • Short-term memory loss • Clumsiness • Balance problems • Depression
Serious complications • Other serious complications can include: • Brain damage • Epilepsy • Changes in eye sight
Vaccine for meningitis~~ • There are vaccines against Hib and against some strains of N. meningitidis and many types of Streptococcus pneumoniae. The vaccine against haemophilus influenze (Hib) has reduced Hib meningitis cases by 95 percent since 1985. • There are vaccines to prevent meningitis due to S. pneumoniae. The pneumococcal polysaccharide vaccine is recommended for all persons over 65 years of age and younger persons at least 2 years old with certain chronic medical problems.
Treatment and prevention of bacterial meningitis • Suspected bacterial meningitis is a medical emergency and immediate diagnostic steps must be taken to establish the specific cause • The mortality rate of untreated bacterial meningitis approaches 100 percent and, even with optimal therapy, there is a high failure rate • Empiric treatment should be begun as soon as the diagnosis is suspected using bactericidal agent(s) that achieve significant levels in the CSF
Use of bactericidal agents • Bactericidal therapy is generally necessary to cure meningitis • Bacteriostatic drugs, such as clindamycin and tetracycline, are inadequate for meningitis • Chloramphenicol is a bacteriostatic drug for most enteric Gram negative rods; however, it is usually bactericidal for H. influenzae, N. meningitidis, and S. pneumoniae and has been extensively and successfully used to treat meningitis caused by these organisms
Choice of agent • Selected third generation cephalosporins such as cefotaxime and ceftriaxone, have emerged as the beta-lactams of choice in the empiric treatment of meningitis • These drugs have potent activity against the major pathogens of bacterial meningitis with the notable exception of listeria • Ceftazidime, another third generation cephalosporin, is much less active against penicillin-resistant pneumococci than cefotaxime and ceftriaxone
Treatment - Empiric • Ceftriaxone 2 gm IV q12h or Cefotaxime 2 gm IV q4-6h • plus Vancomycin 15 mg/kg q6h • If > 50 years, also add Ampicillin 2 gm IV q4h (for Listeria)
THERAPY FOR SPECIFIC PATHOGENS Streptococcus pneumoniae • The conventional approach to the treatment of pneumococcal meningitis was the administration of penicillin alone for two weeks at a dose of four million units intravenously every four hours • Good results have also been obtained with third generation cephalosporins • However, the problem of treating pneumococcal meningitis has recently been compounded by the widespread and increasingly common reports of pneumococcal strains resistant to penicillin
Cefotaxime or ceftriaxone can be used if the MIC for these drugs is less than 0.5 µg/mL • It is recommended that vancomycin (2 g/day) should be given with cefotaxime or ceftriaxone in the initial treatment of pneumococcal meningitis if there has been beta-lactam resistance noted locally • Vancomycin should be continued if there is high level penicillin resistance and an MIC >0.5 µg/mL to third generation cephalosporins • If corticosteroids are given, rifampin should be added as a third agent since it increases the efficacy of the other two drugs • The usual duration of therapy is two weeks
Haemophilus influenzae • A third generation cephalosporin is the drug of choice for H. influenzae meningitis • Patients with H. influenzae meningitis should be treated for five to seven days • For adults, a dose of 2 g every six hours of cefotaxime and 2 g every 12 hours of ceftriaxone is more than adequate therapy • Pharyngeal colonization persists after curative therapy and may require a short course of rifampin if there are other children in the household at risk for invasive Haemophilus infection • The recommended dose is 20 mg/kg per day (to a maximum of 600 mg/day) for four days
Neisseria meningitidis • This infection is best treated with penicillin • Although there are scattered case reports of N. meningitidis resistant to penicillin, such strains are still very rare • A third-generation cephalosporin is an effective alternative to penicillin for meningococcal meningitis • A five day duration of therapy is adequate • However, when penicillin is used, there may still be pharyngeal colonization with the infecting strain. As a result, the index patient may need to take rifampin, a fluoroquinolone, or a cephalosporin
Listeria monocytogenes • Listeria has been traditionally treated with ampicillin and gentamicin, as resistance to these drugs is quite rare • Ampicillin is given in typical meningitis doses (2 g intravenously every four to six hours in adults) and gentamicin is used for synergy • An alternative in penicillin-allergic patients is trimethoprim-sulfamethoxazole (dose of 10/50 mg/kg per day in two or three divided doses) • The usual duration of therapy is at least three weeks
Enteric Gram negative rods • Prior to the availability of third generation cephalosporins, it was often necessary to instill an aminoglycoside antibiotic such as gentamicin directly into the cerebral ventricles • It is now possible to cure these infections with high doses of third generation antibiotics • A repeat CSF sample should be obtained for culture two to four days into therapy to help assess the efficacy of treatment • The duration of therapy should be at least three weeks
PREVENTION OF MENINGITISVaccines A spectacular reduction in H. influenzae meningitis has been associated with the near universal use of a vaccine against this organism in developed countries since 1987 • There has been a 94 percent reduction in H. influenzae meningitis between 1987 and 1995 • Pneumococcal vaccine administered to the chronically ill and elderly is probably useful in reducing the overall incidence of pneumococcal infections. However, its role in the prevention of meningitis is as yet undetermined
Vaccines • Meningococcal vaccines are active against many strains of N. meningitidis • However, the majority of meningococcal infections in the United States are caused by type b meningococcus for which there is no vaccine • Vaccines for other types (notably type a) are recommended for travelers and American military personnel to countries with epidemic meningitis • Immunization against meningococci is not warranted as postexposure prophylaxis
Chemoprophylaxis • There is a role for chemoprophylaxis to prevent spread of meningococcal and haemophilus meningitis but not for pneumococcal disease • The use of antimicrobial therapy to eradicate pharyngeal carriage of meningococci is widely accepted to prevent development of disease in close contacts and to eradicate pharyngeal carriage • Rifampin 600 mg PO every 12 h for a total of four doses is recommended • Ciprofloxacin, in a single dose of 500 mg PO, is equally effective and can be used in patients over the age of 18
Role Of Steroids • The addition of antiinflammatory agents has been attempted as an adjuvant in the treatment of meningitis • Early administration of corticosteroids such as dexamethasone for pediatric meningitis has shown no survival advantage, but there is a reduction in the incidence of severe neurologic complications and deafness • A meta-analysis of five such studies in children showed a relative risk of bilateral deafness of 4.1 and of late neurological sequelae of 3.9 in controls compared to children treated with steroids
A second meta-analysis of trials of meningitis in children evaluated the findings according to organism • For H. influenzae type b meningitis, dexamethasone therapy was associated with a significant reduction in deafness • For pneumococcal meningitis, dexamethasone was effective only if given early ; in this setting, there was a significant reduction in hearing loss • Two days of therapy was as effective and less toxic than longer courses of steroid administration Dexamethasone as adjunctive therapy in bacterial meningitis. A meta-analysis of randomized clinical trials since 1988. JAMA 1997; 278:925
There is no consensus regarding the utility of corticosteroid therapy in adults • The Infectious Disease Society of America considers adjuvant corticosteroids for meningitis to be unsupported for routine use in adults but supports them for H. influenzae infections in children Guidelines for the use of systemic glucocorticoids in the management of selected infections. J Infect Dis 1992; 165:1
MORTALITY RATE AND LATE SEQUELAE • The prognosis of meningitis is linked to age and the presence of underlying disease • Bacterial meningitis accompanying advanced liver disease, HIV infection, or organ transplantation is likely to be associated with more morbidity and mortality • In addition, the prognosis and complications differ in children and adults
The mortality rates are lowest in children • A meta-analysis of prospectively enrolled cohorts of children in developed countries showed a 4.8 percent mortality from 1955 to 1993 • The mortality rate varied by organism, ranging from 3.8% for H. influenzae to 7.5 percent for N. meningitidis to 15.3% for S. pneumoniae • 83.6 percent of the surviving children had apparently complete recovery • The most common sequelae were • Deafness – 10.5 percent. • Bilateral severe or profound deafness – 5.1 percent. • Mental retardation – 4.2 percent. • Spasticity and/or paresis – 3.5 percent. • Seizures – 4.2 percent.
Complications are more common in adults • A series of 86 adults with meningitis, for example, showed a mortality rate of 18.6 percent with a complication rate of 50 percent • The most common problems were: • Cerebrovascular involvement – 15.1 percent. • Cerebral edema – 14 percent. • Hydrocephalus – 11.6 percent. • Septic shock – 11.6 percent. • Disseminated intravascular coagulation – 8.1 percent. • Acute respiratory distress syndrome – 3.5 percent. Spectrum of complications during bacterial meningitis in adults. Results of a prospective clinical study. Arch Neurol 1993; 50:575
A second review of bacterial meningitis in adults from 1962 to 1988 found a mortality rate of 25 percent that did not vary during the 26 years of the study • As in children, there was a higher rate of death due to S. pneumoniae (37 percent) as compared to N. meningitidis (13 percent) and listeria (10 percent) Acute bacterial meningitis in adults. N Engl J Med 1993; 328:21.
THANK YOU!QUESTIONS? Even my family has stopped listening to me! Love is unconditional with Nora