Bacterial Meningitis
Bacterial Meningitis. Presented by, Afrah Abdul Wahid Ali Ashutosh Wanchu Lavina Loungani Sophie Gorniewicz Tahir Yahya. Case Study.

Bacterial Meningitis
E N D
Presentation Transcript
Bacterial Meningitis Presented by, Afrah Abdul Wahid Ali Ashutosh Wanchu Lavina Loungani Sophie Gorniewicz Tahir Yahya
Case Study • A 3 yr old girl was brought to the emergency room by her parents because of fever and loss of appetite for the past 24 hrs and difficulty in arousing her for the past 2 hrs. • The developmental history had been normal since birth. Her childhood immunization were current. • She attended a day care center and had a history of several episodes of presumed viral infections similar to those of other children at the center.
Clinical Features Temperature was 39.5 C Pulse-130/min Respirations-24/min BP-110/60 mm Hg
Physical Examination Physical examination showed a well-developed and well-nourished child of normal height and weight who was drowsy. When her neck was passively flexed, her legs also flexed (+ve Brudzinski sign, suggesting irritation of meninges). Ophthalmoscopic examination showed no papilledema, indicating that there had been no long-term increase in intracranial pressure. The remainder of her physical examination was normal.
Laboratory Findings • CSF fluid was cloudy. Gram staining showed many polymorphonuclear cells with gram negative diplococci suggestive of neisseria meningitidis. • White blood cell count – 25,000/µL ( markedly elevated), with 88% PMN forms and an absolute PMN count of 22,000/µL (markedly elevated), 6% lymphocytes, and 6% monocytes. • CSF protein was 100 mg/dL (elevated) • Glucose was 15 mg/dL (low, termed hypoglycorrhachia) • Cultures of blood and CSF grew serogroup B N. MENINGITIDIS
What is meningitis • Meningitis is a common name for infections (inflammation) that take place in the meninges surrounding the brain and spinal cord. • One of the most serious forms of meningitis is Meningococcal meningitis. It is caused by Neisseria meningitidis. • An infection with meningococcal bacteria causes a serious, potentially fatal infection called meningococcal disease. You may have heard it referred to as bacterial meningitis. Meningococcal disease can also cause a very serious condition called sepsis (blood poisoning).
Types of meningitis • Aseptic meningitis: caused by viruses (e.g. mumps), SLE, and some types of medications. • Bacterial meningitis: caused by a bacterial infection. Numerous microorganisms may cause bacterial meningitis: • Neiseria meningitidis • Streptococcus pneumoniae • Listeria monocytogenes • Haemophilus influenzae (type B) • Mycobacterium tuberculosis • Group B Streptococci • Escherichia coli
Types of meningitis (cont.) • Viral meningitis: caused by viruses (enterovirus). • Tuberculous meningitis: caused by tuberculosis infection due to Mycobacterium tuberculosis. • Cryptococcal meningitis: caused by infection from a yeast called Cryptococcus (found in soil and bird droppings). Often associated with AIDS. • Neoplastic meningitis: caused by the spread of solid tumors to the brain or spinal cord. • Syphilitic meningitis: due to infection with the bacterium that causes syphilis
Epidemiology • SOURCE & RESERVOIR: • Man • Subclinical infection • carrier (they carry the bacteria in their nose and throat but never become sick) • MODES OF TRANSMISSION: • Close contact with a person who is sick with the disease • Contact with carriers • Living in close quarters, such as college dormitories • Being in crowded situations for prolonged periods of time • Sharing drinking glasses, water bottles, or eating utensils • Kissing, sharing a cigarette
Epidemiology (cont.) • INFECTIOUS MATERIAL: • Nasopharyngeal secretions • PEOPLE AT RISK: • Neonates • Children, teens, and young adults • Elderly • People who have a weakened immune system • AIDS patients are at high risk for Tuberculous meningitis
Etiology • Bacterial meningitis is due most often to hematogenous spread of bacteria to the leptomeninges. • It can also be seen after head trauma as skull fracture through the sinuses. • Local infections such as mastoiditis may also lead to meningitis. • Surgery or CNS infection such as cranial epidural abscess may lead to meningitis.
Etiology (cont.) • Neonates: Group B Streptococci, Escheridia coli, Listeria monocytogenes • Infants: Neissera meningitidis, Haemophilus influenzae, Streptococcus pneumoniae • Children: N. meningitidis, S. pneumoniae • Adults: S. pneumoniae, N. meningitidis, Mycobacteria, Cryptococci
Pathogenesis • Bacteria extend through the wall of blood vessels into the subarachnoid space followed more slowly by neutrophils as the blood brain barrier breaks down. • The combination of bacteria and neutrophils in the subarachnoid space irritates the underlying cerebral cortex causing edema and increased intracranial pressure. • If the meningitis is not treated neutrophils are followed by lymphocytes and macrophages which with the bacteria, cause irritation and degeneration of cranial nerves, production of intimal fibrosis in arteries and fibrosis of the leptomeninges which can lead to cortical infarcts and blockage of the foramina of Lushcka and Magendie with hydrocephalus.
General Gross Description • The brain in purulent meningitis has an opacity of the leptomeninges by neutophils and bacteria. This is seen over the convexity and the base. • The brain is also usually swollen.
General Microscopic Description • In acute purulent meningitis, the subarachnoid space is filled with neutrophils and bacteria with increasing numbers of macrophages and lymphocytes over time. • The underlying brain is usually protected by the pia so that there is no intracerebral inflammation, however, the cortex and white matter will show spongy change or vacuolization due to edema. • Infants more often show bacteria and neutrophils invading the underlying parenchyma.
Symptoms • Sudden high fever : The infection causes a high fever of about 130F or more which does not get lower with a tepid bath or fever reducing medicine • Severe, persistent headache • Neck stiffness and pain that makes it difficult to touch your chin to your chest is due to the swelling around the Meninges • Nausea and vomiting, sometimes along with diarrhea • Confusion and disorientation (acting "goofy") can progress to stupor, coma, and death • Drowsiness or sluggishness • Eye pain or sensitivity to bright light • Muscle or joint pain or weakness
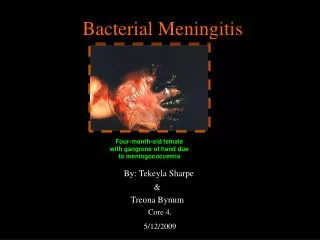
Symptoms • Abnormal skin color • Reddish or brownish skin rash or purple spots that do not turn white when u press on them are a sign of sepsis. These may develop because of inflammation and bleeding in small blood vessels throughout the body, including those under the skin. • Ice-cold hands and feet • Numbness and tingling: Sepsis (also called blood poisoning) can reduce the amount of blood that gets to the persons hand and feet, causing coldness and numbness. • Seizures: Swelling of brain tissue, increases pressure inside the skull, and hampers blood flow, causing stroke symptoms, paralysis and seizures.
Glass Test • Press the side of the glass tumbler against the rash • If the rash does not disappear then it is a symptom of meningitis.
Symptoms In Children • Severe high fever • Feeding problems • Vomiting • Irritability • Seizures • High-pitched crying • Decreased appetite • The skin over the fontanelles (soft spots between the skull bones) becomes taut, and the fontanelles may bulge. • Infants may not develop a stiff neck
Diagnosis WHEN TO CALL THE DOCTOR: • If a child 2 years old or younger has an unexplained fever and the parent senses that the child is ill. • If a child becomes increasingly irritable or unusually sleepy, refuses to eat, vomits, has seizures, or develops a stiff neck. • If an adult has fever, headache, skin rash, confusion, unresponsiveness (stupor), seizures, and a stiff neck.
Diagnosis (cont.) KERNIG SIGN: • The Kernig sign is positive if pain in the lower back or posterior thigh occurs when the knee is extended while the patient is lying in the supine position and the hip is flexed at a right angle.
Diagnosis (cont.) BRUDZINSKI SIGN: • The Brudzinski sign is positive if knee and hip flexion occurs when the neck is flexed while the patient is in the supine position.
Diagnosis (cont.) NECK STIFFNESS: • Nuchal rigidity is typically assessed with the patient lying supine, and both hips and knees flexed. INVESTIGATIONS DONE: • Blood test • Chest X-ray • CSF analysis • CT scan or MRI (MRI preferred over CT due to its superiority in demonstrating areas of cerebral edema, ischemia, and meningeal inflammation) • Cultures of samples of CSF, blood, urine, mucus from the nose and throat, and pus from skin infections.
Diagnosis (cont.) CSF ANALYSIS: • A spinal tap (lumbar puncture) is performed. A thin needle is inserted between L4/L5 to withdraw a sample of CSF. • The sample of CSF is sent to a laboratory, where the bacteria can be cultured and identified. • 3 tubes of CSF are collected • One for chemistry analysis for glucose & protein levels and cell count • One for microbiology analysis for Gram stain, bacterial culture… • One for cytology analysis • It will help doctors distinguish between the different type of meningitis.
Diagnosis (cont.) • Culture media used for bacterial culture of CSF are: • 5% sheep blood agar • Enriched chocolate agar • Enrichment broth (eg, thioglycolate) • Culture plates should be incubated in an atmosphere containing 5 to 10% CO2. • Antimicrobial susceptibility testing should be performed on all clinically relevant bacteria isolated from CSF, so that the antibiotic therapy that was started immediately can be adjusted if necessary.
Diagnosis (cont.) • METHODS FOR DETECTING BACTERIA IN CSF: • Gram staining • Acridine orange stain • Fluorochrome stain (bacteria appear bright red) • More sensitive than gram stain • Reduction in the time of examination of CSF smear • Requires fluorescence microscope • Wayson stain • Simple & sensitive stain for screening CSF smears for bacteria • Bacteria appear dark blue
Diagnosis (cont.) • Quellung procedure (Quellung capsular reaction) • Used to confirm presence of S.pneumoniae, N.meningitidis, or H.influenzae • Antisera specific for the capsular polysaccharides of each of these 3 bacteria are mixed with separate portions of clinical specimens. • Formation of Ag/Ab complexes on the surfaces of these bacteria induces changes in the refractive indices of their capsules. • The capsules appear clear & swollen.
Diagnosis (cont.) • METHODS FOR DETECTING BACTERIAL ANTIGENS: • CIE (counterimmunoelectrophoresis) • COAG (coagglutination) • LA (latex agglutination) • OTHER METHODS USED: • EIA (enzyme immunoassays) • LAL Assay (limulus amebocyte lysate assay) • GLC (gas-liquid chromatography) • PCR (polymerase chain reaction)
Complications If the disease is left untreated, the following manifestatations are seen: Increased spinal fluid pressure Myocarditis: inflammation of the heart Hydrocephalus (blockage of spinal fluid in brain) Mental retardation Deafness :Loss of hearing from infiltration of the 8th nerve Brain damage:Spread from the meninges to the brain is called meningoencephalitis Severe diarrhea and vomiting Internal bleeding Low blood pressure Shock Death
Complications Waterhouse-Friderichsen syndrome Adrenal gland failure due to bleeding into the adrenal gland. Symptoms include acute adrenal gland insufficiency and profound shock. It is deadly if not treated immediately
Treatment • Because bacterial meningitis is a medical emergency, it's important to start the treatment as soon as it is diagnosed or even suspected. • Bacterial meningitis is treated with antibiotics. The doctor will start intravenous (IV) antibiotics with a corticosteroid (eg, Dexamethasone) to bring down the inflammation before all the test results are even known. When the specific bacteria are identified, he may decide to change antibiotics or not. • In addition to antibiotics, it is important to replenish fluids lost from fever, loss of appetite, sweating, vomiting and diarrhea.
Treatment (cont.) • Some patients may need to stay in the hospital, depending on the severity of the illness and the treatment needed. • Complications can require additional treatment. • Anticonvulsants (eg, Diazepam or Phenytoin) might be given for seizures. • Additional IV fluids in case of shock or low blood pressure. • Supplemental oxygen or mechanical ventilation if the child has difficulty breathing. • All neonates should have a hearing test following their recovery to screen for hearing impairment.
Prognosis • If treated immediately, most patients who have acute bacterial meningitis recover fully. • But when diagnosis or treatment is delayed, permanent brain damage or death becomes more likely, especially in very young children and older people. • Some patients develop seizures that require lifelong treatment. • Even with appropriate treatment, about 5-15% patients die from bacterial meningitis. • 10-20% of patients who survive bacterial meningitis have brain damage, hearing problems, or developmental difficulties (especially in children).
Prevention • Cases of bacterial meningitis should be reported to state or local health authorities so that they can follow and treat close contacts of patients and recognize outbreaks. • Overseas travelers should check to see if meningococcal vaccine is recommended for their destination. Travelers should receive the vaccine at least 1 week before departure, if possible.
Prevention (cont.) IMMUNIZATION: • Haemophilus influenzae type b (Hib) vaccine • Part of the recommended immunization schedule in children. • 3 doses given at 2, 4 and 6 months of age, a booster dose is given at 12-15 months of age. • Pneumococcal conjugate vaccine (PCV7) • Recommended for children under 2-5 years old who are at high risk of pneumococcal disease (weak immune system). • 4 doses given at 2, 4, 6 and 12-15 months of age.
Prevention (cont.) • Pneumococcal polysaccharide vaccine (PPV) • Recommended for adults >65 and children >2 years who have long-term health problems. • 1 dose is given (under some circumstances a 2nd dose may be given). • Meningococcal conjugate vaccine (MCV4) • Recommended for children from 11 to 18 years who haven't yet been vaccinated, who are at high risk of bacterial meningitis, for microbiologists, for overseas travelers. • 1 dose is given.
Prevention (cont.) CHEMOPROPHYLAXIS: • Rifampin is given to family members of an infected person to reduce their risk of contracting the disease asH influenzae can persist in the nasopharyngeal secretions even after a successful treatment. • Pregnant women should not take rifampin as it may harm the fetus. They should be treated with single doses of ciprofloxacin, azithromycin, or ceftriaxone.
Tuberculous meningitis DEFINITION: • Infection of the meninges caused by Mycobacterium tuberculosis (acid-fast Gram-positive mycobacterium), the bacteria that causes tuberculosis. • It is the most severe form of tuberculosis. • It is caused by the spread of Mycobacterium tuberculosis to the brain, from another site in the body. Infection begins in the lungs and may spread to the meninges by a variety of routes.
Tuberculous meningitis (cont.) EPIDEMIOLOGY: • In areas with much tuberculosis, • tuberculous meningitis usually affects young children • it develops after the primaty tuberculosis infection • In areas with less tuberculosis, • tuberculous meningitis tends to strike adults. • it is due to reactivation of an old focus of tuberculosis that had been dormant
Tuberculous meningitis (cont.) RISK FACTORS: • history of pulmonary tuberculosis • excessive alcohol use • AIDS • other disorders that compromise the immune system
Tuberculous meningitis (cont.) SYMTOMS:(usually begin gradually) • Fever • Sluggishness • Loss of appetite • Severe headache • Nausea and vomiting • Stiff neck • Sensitivity to light (Photophobia) • Loss of consciousness
Tuberculous meningitis (cont.) DIAGNOSIS: • CSF analysis • Chest radiography • CT scan or MRI • Sputum examination • Sputum culture • Tuberculin skin testing