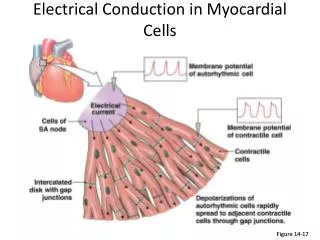
Electrical Conduction in Myocardial Cells
Electrical Conduction in Myocardial Cells . Figure 14-17. 1. 1. SA node. AV node. 2. 1. THE CONDUCTING SYSTEM OF THE HEART. SA node depolarizes. 2. Electrical activity goes rapidly to AV node via internodal pathways. SA node. 3. Internodal pathways. 3. Depolarization spreads

Electrical Conduction in Myocardial Cells
E N D
Presentation Transcript
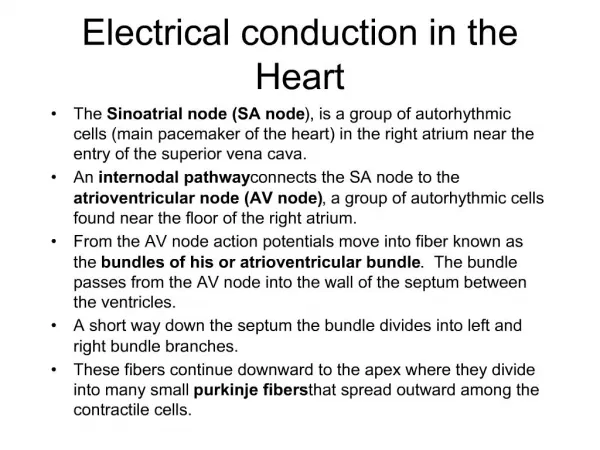
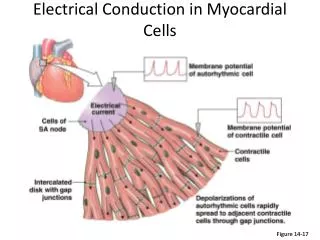
Electrical Conduction in Myocardial Cells Figure 14-17
1 1 SA node AV node 2 1 THE CONDUCTING SYSTEM OF THE HEART SA node depolarizes. 2 Electrical activity goes rapidly to AV node via internodal pathways. SA node 3 Internodal pathways 3 Depolarization spreads more slowly across atria. Conduction slows through AV node. AV node 4 Depolarization moves rapidly through ventricular conducting system to the apex of the heart. A-V bundle 4 Bundle branches Purkinje fibers Depolarization wave spreads upward from the apex. 5 5 Purple shading in steps 2–5 represents depolarization. Electrical Conduction in Heart
1 1 SA node AV node 1 THE CONDUCTING SYSTEM OF THE HEART SA node depolarizes. SA node Internodal pathways AV node A-V bundle Bundle branches Purkinje fibers Purple shading in steps 2–5 represents depolarization. Electrical Conduction in Heart The electrical signal for contraction begins when the SA node fires an action potential and the depolarization spreads to adjacent cells through gap junctions Figure 14-18, step 1
1 1 SA node AV node 2 1 THE CONDUCTING SYSTEM OF THE HEART SA node depolarizes. 2 Electrical activity goes rapidly to AV node via internodal pathways. SA node Internodal pathways AV node A-V bundle Bundle branches Purkinje fibers Purple shading in steps 2–5 represents depolarization. Electrical Conduction in Heart Electrical conduction is rapid through the internodal conducting pathways , but slower through the contractile cells of the atria Figure 14-18, steps 1–2
1 1 SA node AV node 2 1 THE CONDUCTING SYSTEM OF THE HEART SA node depolarizes. 2 Electrical activity goes rapidly to AV node via internodal pathways. SA node 3 Internodal pathways 3 Depolarization spreads more slowly across atria. Conduction slows through AV node. AV node A-V bundle Bundle branches Purkinje fibers Purple shading in steps 2–5 represents depolarization. Electrical Conduction in Heart Figure 14-18, steps 1–3
1 1 SA node AV node 2 1 THE CONDUCTING SYSTEM OF THE HEART SA node depolarizes. 2 Electrical activity goes rapidly to AV node via internodal pathways. SA node 3 Internodal pathways 3 Depolarization spreads more slowly across atria. Conduction slows through AV node. AV node Depolarization moves rapidly through ventricular conducting system to the apex of the heart. 4 A-V bundle 4 Bundle branches Purkinje fibers Purple shading in steps 2–5 represents depolarization. Electrical Conduction in Heart Figure 14-18, steps 1–4
1 1 SA node AV node 2 1 THE CONDUCTING SYSTEM OF THE HEART SA node depolarizes. 2 Electrical activity goes rapidly to AV node via internodal pathways. SA node 3 Internodal pathways 3 Depolarization spreads more slowly across atria. Conduction slows through AV node. AV node 4 Depolarization moves rapidly through ventricular conducting system to the apex of the heart. A-V bundle 4 Bundle branches Purkinje fibers Depolarization wave spreads upward from the apex. 5 5 Purple shading in steps 2–5 represents depolarization. Electrical Conduction in Heart Why is it necessary to direct the electrical signals through the AV node? Why not allow them to spread downward from the atria?
FIBRILLATION If myocardial cells contract in a disorganized manner-fibrillation results. Atrial fibrillation –Not a immediateemergency condition. Ventricular fibrillation,- is an immediately life-threatening emergency. • Treatement- • electrical shock to the heart. The shock creates a depolarization that triggers action potentials in all cells simultaneously, coordinating them again.
Electrical Conduction • AV node • Direction of electrical signals • Delay the transmission of action potentials • SA node • Set the pace of the heartbeat at 70 bpm • AV node (50 bpm) and Purkinje fibers (25-40 bpm) can act as pacemakers under some conditions
Complete heart block- The conduction of electrical signals from the atria to the ventricles through the AV node is disrupted. The SA node fires at its rate of 70 beats per minute, but those signals never reach the ventricles. So the ventricles coordinate with their fastest pacemaker. Because ventricular autorhythmic cells discharge only about 35 times a minute, the rate at which the ventricles contract is much slower than the rate at which the atria contract. • If ventricular contraction is too slow to maintain adequate blood flow, it may be necessary for the heart's rhythm to be set artificially by a surgically implanted mechanical pacemaker. These battery-powered devices artificially stimulate the heart at a predetermined rate.
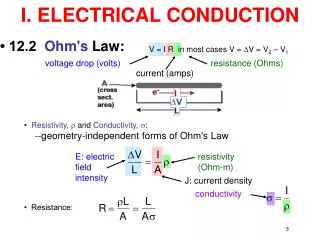
Electrocardiography: Introduction • Body fluids are good conductors (the body is a volume conductor) • Fluctuations in potential (action potentials of myocardial fibers) can be recorded extracellularly • The record of these potential fluctuations during the cardiac cycle is the electrocardiogram (ECG) • The ECG provides information on: - • -Heart rate and rhythm - The pattern of electrical activation of the atria and ventricles - The approximate mass of tissue being activated - Possible damage of the heart muscle - Possible changes in the body’s electrolyte composition
Basic Concept One in Electrocardiography: The ECG reflects changes in the charge on the surface of the heart • When a heart cell is at rest, the inside of the cell is negative relative to the outside, which is positive • However, when an action potential is generated, the inside becomes positive and the outside negative • So, at rest, the outside of the heart is positive, but as an action potential passes, the surface becomes negative • This change in surface charge is recorded in an ECG
Since the AP begins at the SA node, this is the first part of the heart where the surface becomes negative. The rest of the heart is still at rest so its surface is still positive • This produces a charge difference on the surface (between the negative SA node and the other positive parts of the heart) • The difference in surface charge between two areas of the heart is equivalent to oppositely charged poles (known as a dipole). One pole at the SA node would be negative and the other pole at the ventricle would be positive • As the AP is conducted through the remainder of the heart there is an associated wave of negative charge that sweeps over the surface of the heart
Fig. 2. Principles of the bipolar recording of an action potential
If recording electrodes are placed over different points of the body, they will measure this difference in surface charge • When the SA node repolarizes, the heart surface will once again become positive above the SA node, but will still be negative in the remainder of the heart • This will cause the dipole to reverse. Now the positive end is over the SA node and the negative end is over the ventricle
Recording the Electrocardiogram. Basic concept two in Electrocardiography: When the wave of depolarization moves toward the positive electrode, an upward deflection is recorded, whereas depolarization moving in the opposite direction produces a negative deflection • Einthoven’s triangle • hypothetical triangle created around the heart when electrodes are placed on both arms and the left leg .The sides of the triangle are numbered to correspond with the three leads ("leeds"), or pairs of electrodes.
Einthoven’s Triangle Figure 14-19
Important features of the ECG are the P wave, the QRS complex and T wave. • Relevant intervals and segments are the PR interval, the RR interval, the QT segment and the ST segment.
P wave: Atrial depolarization as recorded from the surface of the body P – R interval: Time taken for the wave of depolarization to move through the atria, AV node, bundle of His, Purkinje fibres to the ventricular myocardium. QRS complex: Depolarization of the ventricles. ST segment: Marks the end of the QRS complex and the beginning of the T wave. It occurs when the ventricular cells are in the plateau phase of the action potential (i.e. there is no change in potential occurring and so the ECG baseline is at zero potential) T wave: Repolarization of the ventricles (due to potential changes occurring during phase 3 of the cardiac action potential) Q – T interval: Period during which ventricular systole occurs R – R interval: This time is usually used to calculate the heart rate.
Waves and normal values • P wave- Atrial depolarization 0.1 seconds 0.25 milli volts • PR interval- AV nodal delay 0.12 seconds- 0.2 seconds • QRS complex- ventricular depolarization 0.1-0.11 seconds
EKG Leads Leads are electrodes which measure the difference in electrical potential between either: 1. Two different points on the body (bipolar leads) 2. One point on the body and a virtual reference point with zero electrical potential, located in the center of the heart (unipolar leads)
EKG Leads The standard EKG has 12 leads: 3 Standard Limb Leads 3 Augmented Limb Leads 6 Precordial Leads The axis of a particular lead represents the viewpoint from which it looks at the heart.
Lead I measures the electrical activity between right arm and left arm the electrical activity from right arm to left arm is shown as positive deflection in this lead • Lead II right arm and left leg electrical activity in this direction is shown as positive • Lead III left arm and left leg electrical activity in this direction is shown as positive
Augmented limb leads • Represented by aVR, aVF, aVR. a- augmented V-unipolar Last letter represents the part of body • aVR- between right arm and left arm+ left leg • aVL- between left arm and rt arm+ left leg • aVF- between left foot and rt arm+ lt arm
Precordial Leads Adapted from: www.numed.co.uk/electrodepl.html
Pre cordial leads • V1- 4th intercoastal space, rt side sternal boarder • V2- 4th intercoastal space lt side of sternal boarder • V3- between V2 and V4 • V4- 5th intercoastal space in the mid clavicular space • V5- 5th intercoastal space in the anterior axillary line • V6- 5th intercoastal space in the mid axillary line.
Determining the Heart Rate • Rule of 300 • 10 Second Rule
Rule of 300 Take the number of “big boxes” between neighboring QRS complexes, and divide this by 300. The result will be approximately equal to the rate Although fast, this method only works for regular rhythms. Alternatively, count the number of small boxes between neighboring QRS complexes, and divide 1500 by this number.
What is the heart rate? www.uptodate.com (300 / 6) = 50 bpm (1500/30) = 50 bpm
What is the heart rate? www.uptodate.com (300 / ~ 4) = ~ 75 bpm (1500/20 ) = 75 bpm
What is the heart rate? (300 / 1.5) = 200 bpm
The Rule of 300 It may be easiest to memorize the following table:
The QRS Axis The QRS axis represents the net overall direction of the heart’s electrical activity. Abnormalities of axis can hint at: Ventricular enlargement Conduction blocks (i.e. hemiblocks)
The QRS Axis By near-consensus, the normal QRS axis is defined as ranging from -30° to +90°. -30° to -90° is referred to as a left axis deviation (LAD) +90° to +180° is referred to as a right axis deviation (RAD)
Determining the Axis • The Quadrant Approach • The Equiphasic Approach
Cardiac vector • The cumulative direction of the action potentials in the cardiac muscle • If the vector is directed towards the lead, positive deflection on ECG of that lead • If the vector is directed away from the lead, negative deflection on ECG of that lead • If the vector is directed perpendicular to the direction of the lead, equiphasic ECG of that lead
Determining the Axis Predominantly Positive Predominantly Negative Equiphasic