Download

1 / 120
1.22k likes | 1.47k Vues
Advantages of renin-angiotensin system blockade in the treatment of cardiovascular disease. V. Gerc Clinic for Heart Disease and Rheumatism Sarajevo. The cardiovascular continua in cardiovascular disease. The pathophysiological continua in cardiovascular disease.

E N D
Advantages of renin-angiotensin system blockade in the treatmentof cardiovascular disease V. Gerc Clinic for Heart Disease and Rheumatism Sarajevo
The pathophysiological continua in cardiovascular disease
Angiotensin II is central to atherosclerotic mechanisms Oxidative Stress Inflammation NAD(P)H oxidase activity ↑ Vascular permeability ↑ Leucocyte infiltration ↑ Reactive oxygen species ↑ Activation of signalling pathways LDL peroxidation ↑ Production of inflammatory mediators Angiotensin II LDL peroxidation ↓ Nitric oxide ↓ Proliferation of VSMCs Vasoconstriction Matrix deposition PAI-1 activation Platelet aggregation MMP activation Endothelial dysfunction Tissue remodelling Schmieder et al. Lancet 2007;369:1208−1219
Vascular Risk Factors and Endothelial Dysfunction Role of oxidative stress: Angiotensin II Smoking Hypertension Homocysteine oxLDL Diabetes oxidative stress - - Bradykinin/NO Antioxidants (?) Endothelial Dysfunction mod. from Gibbons GH, Clin Cardiol 20 (1997)
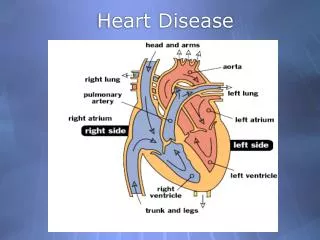
Mechanism of action of angiotensin-converting enzyme inhibitors
EFFECTS OF ANGITENSIN II • vasoconstriction (”afterload” ) • reabsorption of Na+ and water (“preload” ) • coronary constriction • syntesis of cellular proteins (HLV) • fibroblastic hyperplasia (myocardial fibrosis) • apoptosis of myocites • diastolic dysfunction of the heart
EFFECTS OF ANGIOTENSIN II • sympathetic, vagal activity • adrenocortex ( catecholamine, aldosterone) • endothelial dysfunction • PAI-1 ( fibrinolysis) • tissue factor • proliferation and migration of smooth muscles
Potential pathogenic propertiesof Angiotensin II • Heart • Myocardial hypertrophy • Interstitial fibrosis
Potential pathogenic propertiesof Angiotensin II • Coronary Arteries • Endothelial dysfunction with decreased release of nitric oxide • Coronary constriction via release of noradrelanine • Increased oxidative stress; oxygen derived free radicals formed via NADH • Promotion of inflamatory response and atheroma
Potential pathogenic propertiesof Angiotensin II • Kidneys • Increased intraglomerular pressure • Increased protein leak • Glomerular growth and fibrosis • Increased sodium reabsorption
Potential pathogenic propertiesof Angiotensin II • Adrenals • Increased formation of aldosterone
Potential pathogenic propertiesof Angiotensin II • Coagulation system • Increased fibrinogen • Increased PAI-1
Inhibition of the RAS • Inhibition of the RAS is established for the treatment and now prevention of a wide range of cardiovascular disease. The basic concept hinges on the adverse effects of excess angiotensin II and increase protective bradykinin.
Renin – Angiotensin - Aldosterone system: where inhibitors act
Dual role of ACE inhibitors, both preventing and treating cardiovascular disease
Indications for ACEI, based on trial data • 1.Heart failure, all stages • 2. Hypertension • 3.AMI, postinfarct LV dysfunction • 4.Nephropathy, nondiabetic and diabetic • 5. Diabetes type 2, lessens new microalbuminuria and LV hypertrophy
Antiatherosclerotic effect of LISINOPRIL Blood pressure Reduction of cardiovascular events Oxidative stress Inflammation Endothelian dysf. Nitric oxide Growth of the plaque Fibrinolysis tPA PAI-1 ACE
Angiotensin-converting enzyme inhibitors in hypertensive patients at high cardiovascular risk ACEI
ACE inhibitors in hypertension • ACEI are effective as monotherapy in BP reduction in most patients. There are few side effects and contraindication
ACE inhibitors in hypertension • A particulary attractive combination is that with diuretics, because diuretics increase circulating renin activity and angiotensin II levels, wich ACEI counterregulate by inhibiting the conversion of angiotensin I to angiotensin II.
Role of ARB in the treatment of cardiovascular diseases, with a special reference to LOSARTAN
Arguments favoring development of ARBs • ACE inhibitors are not specific • ACE inhibitors do not provide • complete blockade of RAS • Alternative pathways for angiotensin • II formation • Significant incidence of cough
Arguments favoring development of ARBs • ACE inhibitors are not specific • ACE inhibitors do not provide • complete blockade of RAS • Alternative pathways for angiotensin • II formation • Significant incidence of cough
100 80 60 40 20 0 Angiotensin II formation in the heart mediated by chymase v.s. formation mediated by angiotensin converting enzyme ACE mediated Chymase mediated A II formation, % Rat Mouse Rabbit Dog Human Balcells E, et al. Am J Physiol. 1997;273:H1769–H1774.
100 80 60 40 * 20 * * * * * * * 0 30 20 10 * 0 Placebo 4 h 24 h 1 2 3 4 5 6 Hospital Months “Escape”of angiotensin II despite ACE inhibition Plasma ACE (nmoL/mL/min) Plasma Ang II (pg/mL) Biollaz J, et al. J Cardiovasc Pharmacol. 1982;4(6):966-972. *P <.001 vs placebo
Inhibition of the RAS • ARBs directly block the angiotensin II receptor (AT1), thereby largely avoiding the side effects of excess bradykinin such as cough and angioedema.
Effects of Angiotensin II upon AT1i AT2receptors AT1 AT2 Vasodilation Antiproliferative effect Apoptosis Antidiuresis/antinatriuresis Bradykinin formation Release of NO Vasoconstriction Aldosteron release Oxidative stress Vasopresin release Activation of SNS Inhibition of renin release Renal reabsorption ofNa+i H2O Cell growth and proliferation Siragy H. Am J Cardiol. 1999;84:3S-8S.
ARBsIndications • Hypertension • Heart failure • Secondary prevention following myocardial infarction • Diabetic nephropathy • Proteinuria/microalbuminuria • Left ventricle hypertrophy • Atrial fibrilation • Cough caused by ACEI
Studies with Losartan The Losartan Heart Failure n=722Study (ELITE) The Losartan Hypertension n=9194Survival Study (LIFE) The Losartan Heart Failure n=3152Survival Study (ELITE II) The Losartan Post-MI Survival n=5000Study (OPTIMAAL) The Losartan Renal Protection n=1520Study (RENAAL) 19,588
Andersson, 1998 DP mmHg SP mmHg Plac Los CC CC 50 8 16 Plac Los CC CC 50 8 16 4 4 0 0 -4 -4 -8 -8 * * * # -12 -12 * -16 -16 * * -20 -20 * p<0.001 vs plac ; # p>0.05 vs Los n 85 83 82 84 Comparison of efficacy of candesartan and losartan in the treatment of hypertension : resultsat trough
DP mmHg SP mmHg Plac Los CC CC 50 8 16 Plac Los CC CC 50 8 16 4 4 0 0 -4 -4 -8 -8 * -12 * -12 * -16 -16 * * -20 -20 * * p<0.001 vs plac n 85 83 82 84 Comparison of efficacy of candesartan and losartan in the treatment of hypertension : results at peak Andersson, 1998
Los 50 Amlo 10 Vals 80 Amlo 5 0 0 -4 -4 -8 -8 mmHg SP -12 -12 DP -16 -16 CC 8 Amlo 10 Plac Irbe 75 - 300 Amlo 2.5 - 10 0 0 -4 -4 mmHg -8 -8 -12 -12 -16 -16 Comparison of efficacy of ARBs and amlodipine in the treatment of mild and moderate hypertension
Vals 80 Enal 20 Los 50 Enal 20 0 0 -4 -4 -8 -8 -12 -12 SP -16 -16 DP CC 4- 8 Enal 10-20 Irbe 75-300 Enal 10- 40 0 0 -4 -4 -8 -8 mmHg -12 -12 -16 -16 Comparison of efficacy of ARBs andenalapril in the treatment of mild and moderate hypertension mmHg
0 -4 -8 -12 -16 0 -4 -8 -12 -16 Comparison of efficacy of ARBs andhydrochlorothiazide in the treatment of hypertension Los 50 HCTZ 12.5 Vals 80 HCTZ 25 0 -4 -8 mmHg -12 -16 CC 8 HCTZ 25 SP mmHg DP
Irbes 75-150 Atenolol 50-100 Los 50 Atenolol 50 0 0 -2 -2 -4 -4 -6 -6 -8 -8 -10 -10 -12 -12 -14 SP -14 DijastolniP. DP Comparison of efficacy of ARBs andatenolol in the treatment of mild and moderate hypertension mmHg